SURGICAL ETHICS
Prof. Md.Mazibar Rahman
FCPS, FRCS, FACS, FICS
,
Fellow in urology (Australia)
Professor of Surgery
Popular Medical College Hospital
2.
Ethics – Defined
•The word ethics is derived from the Greek word -
“ethos” which means “ character “.
• To put it formally ethics is the branch of
philosophy that defines what is good for the
individual and for society and establishes the nature
of obligations, or duties, that people owe themselves
and one another.
ETHICS / MORAL
•The oldest scientific and philosophical discipline
• ? Demarcation: science / subject
ethics moral
(gr. ethos = custom, (lat. mos = character,
practice) nature)
- Ethics – discipline about moral or philosophy on
moral
- Moral – system of norms or rules, written or not,
about human behavior
5.
Ethics is aphilosophical discipline
about moral problems, deals with art
of living
7.
What is Ethics?
•The formal study of:
–What is right and wrong.
–The study of the bases or principles for
deciding right and wrong.
–The analyses of the processes by which we
decide what is right and wrong.
9.
Ethics is not:
•Merely obeying the law
• Compliance
Although in many instances laws are
statements of considered ethical
positions and most of the time obeying
the law is an element of ethical
behavior.
10.
Relation between moraland other regulative
norms
- Moral norm – specific individual system of personal
values with validity of genesis, development and
adoption
• Other regulative norms (close to moral):
- Of primitive society
- Of customs
- Of religion
- Of law
11.
• Religious vs.Moral norms:
- religious norms are characterized by concept
“sanctity”
(moral ones by term “good”)
- religious norms are more absolute, without
conditions and inevitable that moral ones
- when broke religious norm, a man committed sin
(when violated moral norm, a man felt he
committed mistake against his dignity)
12.
Traditional arrangements ofthe
field of ethics:
• Meta-ethics (nature of right or good, nature
and justification of ethical issues)
• Normative ethics ( standards, principles)
• Applied ethics (actual application of ethical
principles to particular situation)
14.
Three Broad Typesof Ethical Theory:
• 1) Consequentialist theories (primarily concerned
with the ethical consequences of particular actions)
• 2) Non-consequentialist theories (broadly
concerned with the intentions of the person making
ethical decisions about particular actions)
• 3) Agent-centered theories (more concerned with
the overall ethical status of individuals)
15.
Applied Ethics
• TermsUsed in Ethical Judgments
- Obligatory: it is not only right to do it, but that it is
wrong not to do it (ethical obligation to perform the
action)
- Impermissible: it is wrong to do it and right not to do it
- Permissible: or ethically “neutral,” because it is neither
right nor wrong to do
• Supererogatory: types of actions are seen as going
“above and beyond the call of duty (they are right to
do, but it is not wrong not to do them)
16.
Types of Ethics
•Professional Ethics: Obligations of the profession
- Self-regulation
- Education of self and others
• Medical Ethics:
- human: medical (in narrow sense) and dental
- veterinarian
Knowledge, deliberation, understanding of medical
practice that should be in perspective of right,
honorable, accurate behavior
17.
Medical Ethics
• afield of applied ethics, the study of moral
values and judgments as they apply to
medicine. As a scholarly discipline, medical
ethics encompasses its practical application in
clinical settings as well as work on its history,
philosophy, theology, sociology, and
anthropology.
Based on definition of “Medical Ethics” http://en.wikipedia.org/wiki/Medical_ethics
18.
Why study medicalethics?
• “As long as the physician is a knowledgeable and skilful
clinician, ethics doesn’t matter.”
• “Ethics is learned in the family, not in medical school.”
• “Medical ethics is learned by observing how senior
physicians act, not from books or lectures.”
• “Ethics is important, but our curriculum is already too
crowded and there is no room for ethics teaching.”
19.
Why study medicalethics?
• ethics is and always has been an essential
component of medical practice
• some ethical principles are basic to the physician-
patient relationship, but application in specific
situations is often problematic due to disagreement
about what is the right way to act)
• study of ethics prepares medical students to
recognize difficult situations and to deal with them
in a rational and principled manner
20.
Bioethics
• Medical ethicsclosely related to bioethics
(biomedical ethics), but not identical
- medical ethics focuses primarily on issues arising out
of the practice of medicine
- bioethics: very broad subject, concerned with the
moral issues raised by developments in the
biological sciences
- bioethics does not require the acceptance of certain
traditional values that are fundamental to medical
ethics
22.
Bioethics
• Branch ofapplied ethics that studies the
philosophical, social, and legal issues arising in
medicine and the life sciences
• It is chiefly concerned with human life and
well-being, though it sometimes also treats
ethical questions relating to the nonhuman
biological environment
25.
As Practical Ethics,Medical Ethics
focuses on:
The process of deciding what is the most
appropriate (right) course of action in a
particular situation:
• given these facts
• given my skills and abilities
• operating with finite knowledge
• in real time
• and then effecting that course of action.
26.
Ethical Problems
• Problemscaused by fact of having to choose
between goods or things to which we owe an
obligation
• Bad rankings of goods
• Failure to grasp facts
–Ignorance
–Incompetence
–Willful blindness
• Bad factual analysis
–Often caused by personal or institutional
distortion
27.
Organizational Problems
• Generalorganizational culture
• Ego and narcissism
• Overly punitive responses
• Lack of a culture of responsibility
• Failure to acknowledge information distortion
• Bad communication flows
• High transaction costs for doing the “right”
thing
28.
Process of makingethical decisions
• Awareness—Is there a moral issue here?
–What is its nature? How important?
• What are the facts?
• What are the issues?
• What rules or values apply here?
• To whom or what do I owe a duty?
• How should they be applied?
• Who needs to decide and act? Who ought to?
• To what am I obligated because of role/position?
• What are the consequences?
• What are the options?!
29.
Duties to whomor what?
• Individuals
– Patients
– Patients’ families/guardians
– Colleagues
– Co-workers
– Self
• Groups
– Profession
– Society
– The weak
• Ideas/Principles
– The Law
– Truth
– Justice
– Individual value
30.
Duties—Sources
• Legal Obligations
–Healthinsurance
–Emergency treatment
–Reporting duties
• Institutional Obligations
–Practices of hospital
• Professional norms and obligations
–Inhere with being a physician
31.
Framework for ethicaldecision-making
IN PRACTICE
1. Determine whether the issue at hand is an ethical
one.
2. Consult authoritative sources to see how
physicians generally deal with such issues.
3. Consider alternative solutions.
4. Discuss your proposed solution with those whom it
will affect.
5. Make your decision and act on it.
6. Evaluate your decision and be prepared to act
differently in future.
32.
Factors in ethicaldecision-making in
health-care
1. Ethical theories
2. Ethical principles
3. Ethical rules
33.
ETHICAL MAXIM (principles)
Generalguidelines that site what is forbidden,
desirable or permissible (often base for rules)
1. Respecting autonomy
2. Doing no harm (nonmaleficence)
3. Benefiting others (beneficence)
4. Being just (justice)
- Being faithful (fidelity)
34.
ETHICAL RULES (codes)
Mannersdeveloped by professional organizations
Structure of codes:
1. regulative
2. protective (for public opinion)
3. specific (regarding membership)
4. obligated
36.
Surgical Ethics
Ethics isan essential discipline in the practice of
surgery.
•Represents your best understanding of moral
responsibility.
•Evolves as reasoned reflection on clinical experience.
•Role of the Surgeon is to act as the patient’s fiduciary
(person to whom property or power is entrusted for)
38.
Introduction (1)
• Ethicsand surgical intervention must go hand in
hand.
• Both surgeons and some attempted murderers use
knives to accomplish their goals. What is the
difference?
• Why people are willing to risk allowing surgeons
whom they may not have even met to cut them, at
times in potentially lethal ways?
39.
Introduction (2)
• Ifsomeone deliberately cuts another person, draws blood,
causes pain, leaves scars and disrupts everyday activity
then the likely result will be a criminal charge. If the person
dies as a result, the charge could be manslaughter or even
murder.
• The difference between the criminal and the surgeon is that
the surgeon causes harm only incidentally.
• The surgeon’s intent is to cure or manage illness and any
bodily invasion that occurs only does so with the
permission of the patient.
40.
Questions (1)
• Patientsconsent to surgery because they trust their
surgeons.
1. What should such consent entail in practice
2. What should surgeons do when patients
need help but are unable or unwilling to agree
to it?
41.
When patientsdo consent to treatment, surgeons
exert enormous power over them, the power not just
to cure but to injure, disable and kill.
1. How should such power be regulated to
reinforce the trust of patients and to ensure that
surgeons practice to an acceptable professional
standard?
2. Are there circumstances in which it is
acceptable to sacrifice the trust of individual patients
in the public interest through revealing information
that was communicated in what patients believed to
be conditions of strict privacy?
Questions (1) Contd
42.
Questions (2)
• Thesequestions about what constitutes good
professional practice concern ethics rather than
surgical technique.
• Surgeons may be expert in the management of
specific diseases but may have little understanding
of how much and what sort of information is
required for patients to give valid consent to
treatment.
43.
• Surgeons canunderstand the delicate techniques
associated with specific types of procedures without
necessarily knowing when these should be
administered to patients who are unable to consent at
all.
• Surgeons can recognize their own mistakes and
those of colleagues without knowing how much
should be said about them to others.
Questions (2) Contd
44.
Questions (3)
• Traditionalsurgical training offers little help in
the resolution of such ethical dilemmas.
• Aim: To provide guidance which is morally
coherent, widely endorsed and legally
justifiable.
45.
AUTONOMY
• What makesus unique as animals is our
autonomy, our ability to formulate both
goals and beliefs about how these should be
achieved.
• Humans can attempt to plan their lives on
the basis of reason and choice in ways which
other animals cannot.
46.
AUTONOMY
• When wetalk of the particular type of
respect which it is appropriate to show to
humans, the focus should primarily be on
our autonomy rather than our particular
physical characteristics.
• Respect for human dignity is respect for
human autonomy.
47.
AUTONOMY
• Surgeons havea duty of care towards their
human patients which goes beyond just
protecting their life and health. Their
additional duty of care is to respect the
autonomy of their patients, their ability to
make choices about their treatments and to
evaluate potential outcomes in light of
other life plans.
48.
AUTONOMY
• Patients havethe right to exercise choice
over their surgical care.
• To the degree that patients have a right to
make choices about proposed surgical
treatment, it then follows that they should
be allowed to refuse treatments that they
do not want, even when surgeons think that
they are wrong.
49.
Autonomy
Respect the autonomyof patients & their ability to
make choices about their treatments.
It recognizes rights of patients to self-determination.
So patients have right to make choices over their
surgical care.
Respect for autonomy is the basis for informed
consent and advance directives.
50.
Information
Explanation of thepatient’s disease
Explanation of untreated natural history
Recommendation of most appropriate surgery
Discussion of risks and benefits
Anticipated outcome – prognosis
Treatment alternatives
51.
Consent – principles
Venue– calm & quite place
Consent form – Pt’s language
Time – take own decision
Principal person – Surgeon
Entry – case record
52.
For agreement tocount as consent to treatment, patients need to
be given appropriate and accurate information about:
• Their condition and the reasons why it warrants surgery
• What type of surgery is proposed and how it might correct
their condition
• What the proposed surgery entails in practice
• The anticipated prognosis of the proposed surgery
• The expected side-effects of the proposed surgery
• The unexpected hazards of the proposed surgery
• Any alternative and potentially successful treatments for
their condition other than the proposed surgery, along with
similar information about these
• The consequences of no treatment at all.
53.
INFORMED CONSENT
• Aquiet venue for discussion should be found.
• Written material in the patient’s preferred language
should be provided to supplement verbal
communication.
• Patients should be given time and help to evaluate
their own understanding and to come to their own
decision.
• The person obtaining the consent should ideally be
the surgeon who will carry out the treatment.
54.
INFORMED CONSENT
• Goodcommunication skills go hand in hand with
properly obtaining informed consent for surgery.
• Attention must be paid to:
1. Whether or not the patient has understood
what has been stated
2. Avoiding overly technical language in
descriptions and explanations
3. The provision of translators for patients whose
first language is not English
4. Asking patients if they have further questions.
55.
Attention
Information – accurate& reasonably
complete.
Avoidance – technical language
Provision of Translators
Clarification of doubts
56.
INFORMED CONSENT
• Inlaw, intentionally to touch another person
without their consent is a battery.
• Negligence is the second legal action which might
be brought against a surgeon for not obtaining
appropriate consent to treatment.
• If the patient agrees to proceed, no other treatment
should ordinarily be administered without further
explicit consent.
57.
INFORMED CONSENT
• Theduty of surgeons to respect the autonomy of
patients translates into the specific responsibility to
obtain informed consent to treatment.
• For consent to be valid, patients must:
1. Be competent to give it – to be able to
understand, remember, deliberate about and
believe whatever information is provided to them
about treatment choices.
58.
2. Not beforced into decisions which reflect the
preferences of others rather than themselves.
3. Be given sufficient information for these
choices to be based on an accurate understanding
of reasons for and against proceeding with specific
treatments.
• For consent to be valid, patients must:
INFORMED CONSENT
59.
Practical Difficulties
Refusal orwaiver by patient
Temporary Unconsciousness patients
Children less than 18 yrs are minors and are
legally incompetent.
Incompetence – other kind
60.
End of Life– Issues
In unusual circumstances (close to death) that no
evidence shows that a specific treatment desired by
the patient will provide any benefit from any
perspective, the physician need not provide such
treatment.
If there are no treatment options i.e. the pt is brain
dead and the family insists on treatment – if there is
nothing that the physician can do; treatment must
stop.
Noted in case sheet along with senior clinician’s
agreement
61.
Confidentiality
The principle ofconfidentiality is that the
information a patient reveals to a surgeon is private
and has limits on how and when it can be disclosed to
a third party.
The patient (and the person treating the patient)
have right to dignity.
Breaking confidentiality
- If the patient is threat to self or others
- Other team members – improving treatment options
- Public interest
- Court order
62.
Research
Surgeons have asubsidiary responsibility to
improve operative techniques through research,
to assure their patients that the care proposed
is best.
The administration of such regulation is
through research ethics committees, and
surgeons should not participate in research that
has not been approved by such bodies.
63.
Good Standards
To optimizesuccess in protecting life and health to
an acceptable standard, surgeons must only offer
specialized treatment in which they have been
properly trained.
To do so will entail sustained further education
throughout a surgeon’s career in the wake of new
surgical procedures.
To do otherwise would be to place the interest of
the surgeon above that of their patient, an imbalance
that is never morally or professionally acceptable.
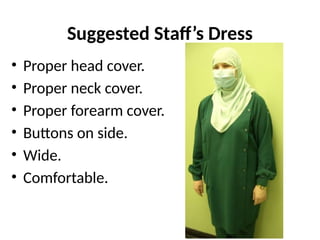
Some Ethical Issuesin The OR
I. Exposure of body.
II. Dress.
III. People gathering and traffic.
IV. Noise.
V. Comments and behavior.
VI. Honesty.
VII. Consent.
Exposure of body
•Parts of body should not be exposed to
others ( governed by religion )
–men : from umbilicus to knees.
–ladies : all body.
• Exceptions are allowed when necessary
according to a definite need.
• Exposure of some body parts is often
necessary, depending on procedure.
68.
Exposure of body- Examples
• Preparation for
anesthesia
• Chest auscultation &
inspection.
• Insertion of folly
catheters.
69.
Exposure of body- Examples
• Patient’s transfer to &
from:
–Operating table,
–Recovery,
–The ward.
70.
Exposure of body- Examples
• Positioning of patient.
• Application of tourniquet.
• Cleaning & draping.
• Removal of draping &
tourniquet.
• Application of cast.
71.
Exposure of body
Wheneverexposure is necessary,
it should be :
• Limited to parts needed only.
• In the presence of limited number of people.
• For the shortest period of time.
72.
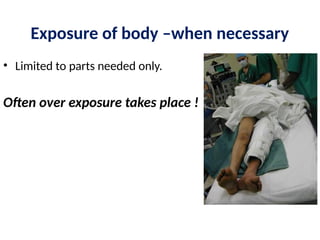
Exposure of body–when necessary
• Limited to parts needed only.
Often over exposure takes place !
73.
Exposure of body- when necessary
• In the presence of limited number of
people.
Often too many people around
(Drs. / Nurses / Technicians / Students/ workers)
Often unnecessary
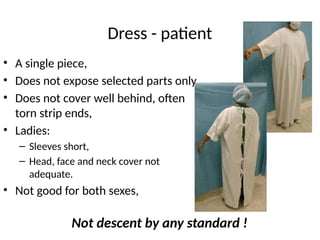
Dress - patient
•A single piece,
• Does not expose selected parts only,
• Does not cover well behind, often
torn strip ends,
• Ladies:
– Sleeves short,
– Head, face and neck cover not
adequate.
• Not good for both sexes,
Not descent by any standard !
79.
Dress - patient
•Underwear by some policies should be
removed
( even if operation is at neck ! ).
• Problems with patient’s underwear :
–uncleanliness / metal parts / nylon ?
• Solution:
–ensure and allow clean underwear.
–Provide proper disposable underwear .
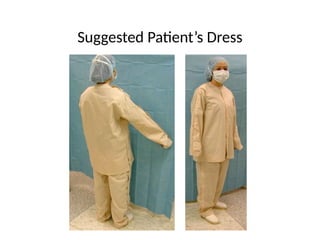
Suggested Patient’s Dress
Criteria
•Should provide adequate cover according
to local standards (religion).
• Should provide adequate local (selective)
exposure.
• Should allow quick & practical wide
exposure in emergency situations.
• Should look descent.
People’s gathering andtraffic
• Often too many people in the corridors, receiving
area & OR causes inconvenience to patients &
staff.
• Problem related to :
- behavior of staff & students.
- limited space.
(Both should be discussed & improved)
Comments & Behavior
•Jokes & laughing:
–Loudly,
–In front of patients,
–In a language not known to them !
–Before anesthesia,
–During procedure with local/spinal
anesthesia.
101.
Comments & Behavior
•Comments & remarks on patient’s:
–Disease,
–Body shape or weight,
–Behavior …etc.
That would not be said if patient is
awake
102.
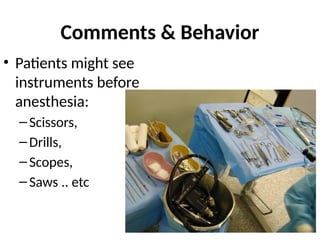
Comments & Behavior
•Patients might see
instruments before
anesthesia:
–Scissors,
–Drills,
–Scopes,
–Saws .. etc
103.
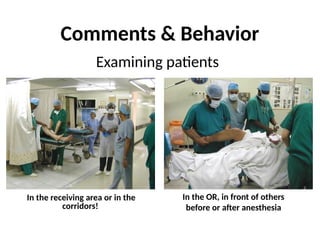
Comments & Behavior
Examiningpatients
In the OR, in front of others
before or after anesthesia
In the receiving area or in the
corridors!
Honesty
• Patients oftenask who performed surgery
• The answer should be honest & concentrate
on :
–Concept of team work.
–Quality is assured.
–Supervised by the consultant / senior staff.
–Teaching / training does not reduce
standards.
• Preserve Patients’dignity during all phases of
transportation.
• Patients should not be exposed unnecessarily
regarding:
–The area exposed,
–The duration of exposure,
–The number of people present during exposure.
• Patient examination if needed should be
inside the operating room only, with privacy
& limited exposure.
Conclusions & Suggestions
108.
• During patientpositioning & preparation should only
allow those whose presence is absolutely necessary :
Allow other staff and students in only after the patient
is draped.
(not just for lady patients)
Conclusions & Suggestions
109.
CONCLUSION
• The twogeneral duties of surgical care are to
protect life and health and to respect autonomy,
both to an acceptable professional standard.
• The specific duties of surgeons are shown to follow
from these: acceptable practice concerning
informed consent, confidentiality, decisions not to
provide, or to omit, life-sustaining care, surgical
research and the maintenance of good
professional standards.
110.
•The final dutyof surgical care is to exercise all of these
general and specific responsibilities with fairness and justice,
and without arbitrary prejudice.
•The conduct of ethical surgery illustrates good citizenship:
protecting the vulnerable and respecting human dignity and
equality.
•To the extent that the practice of individual surgeons is a
reflection of such sustained conduct, they deserve the civil
respect which they often receive.
•To the extent that it is not, they should not practice the
honorable profession of surgery.
CONCLUSION