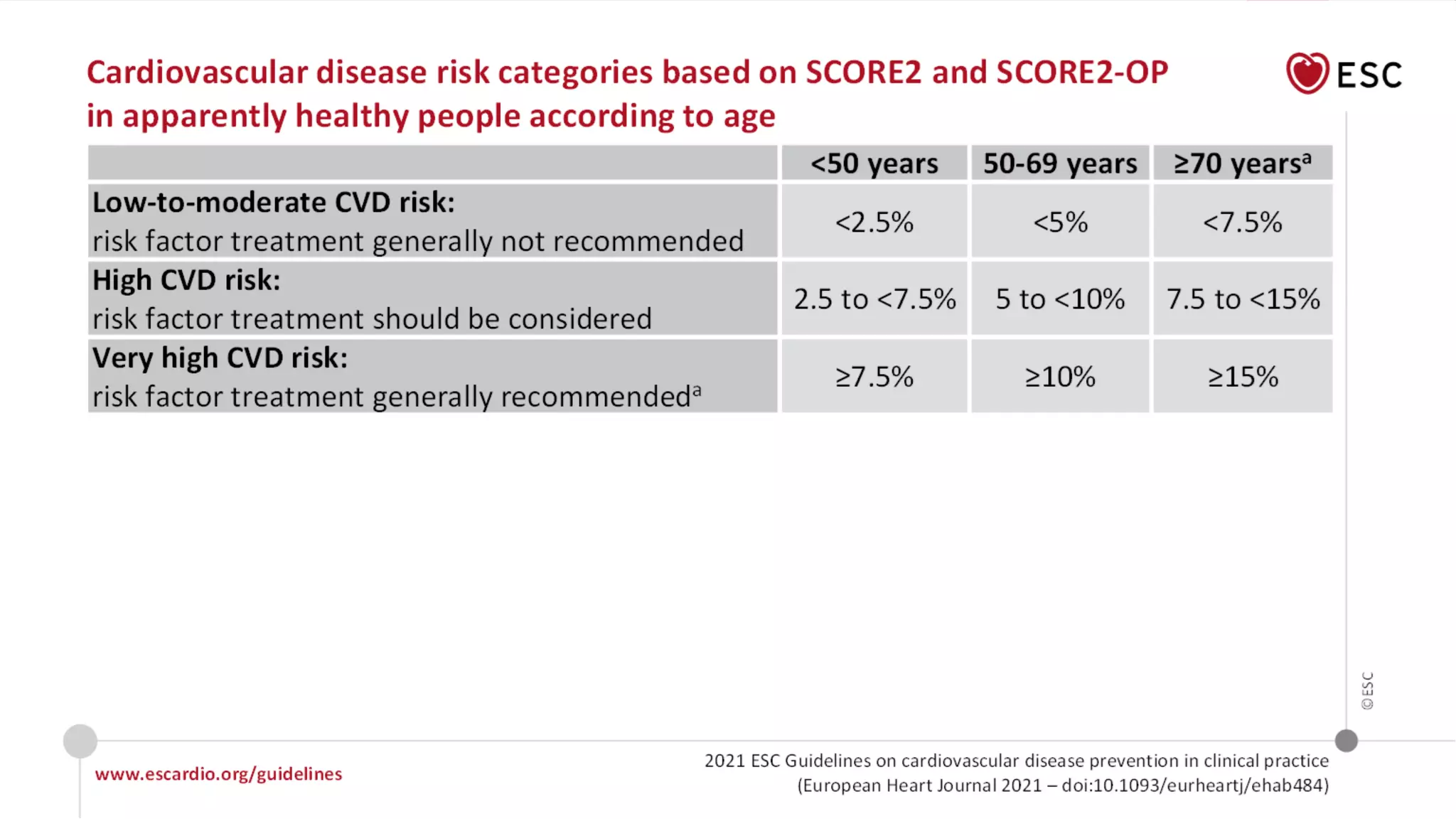
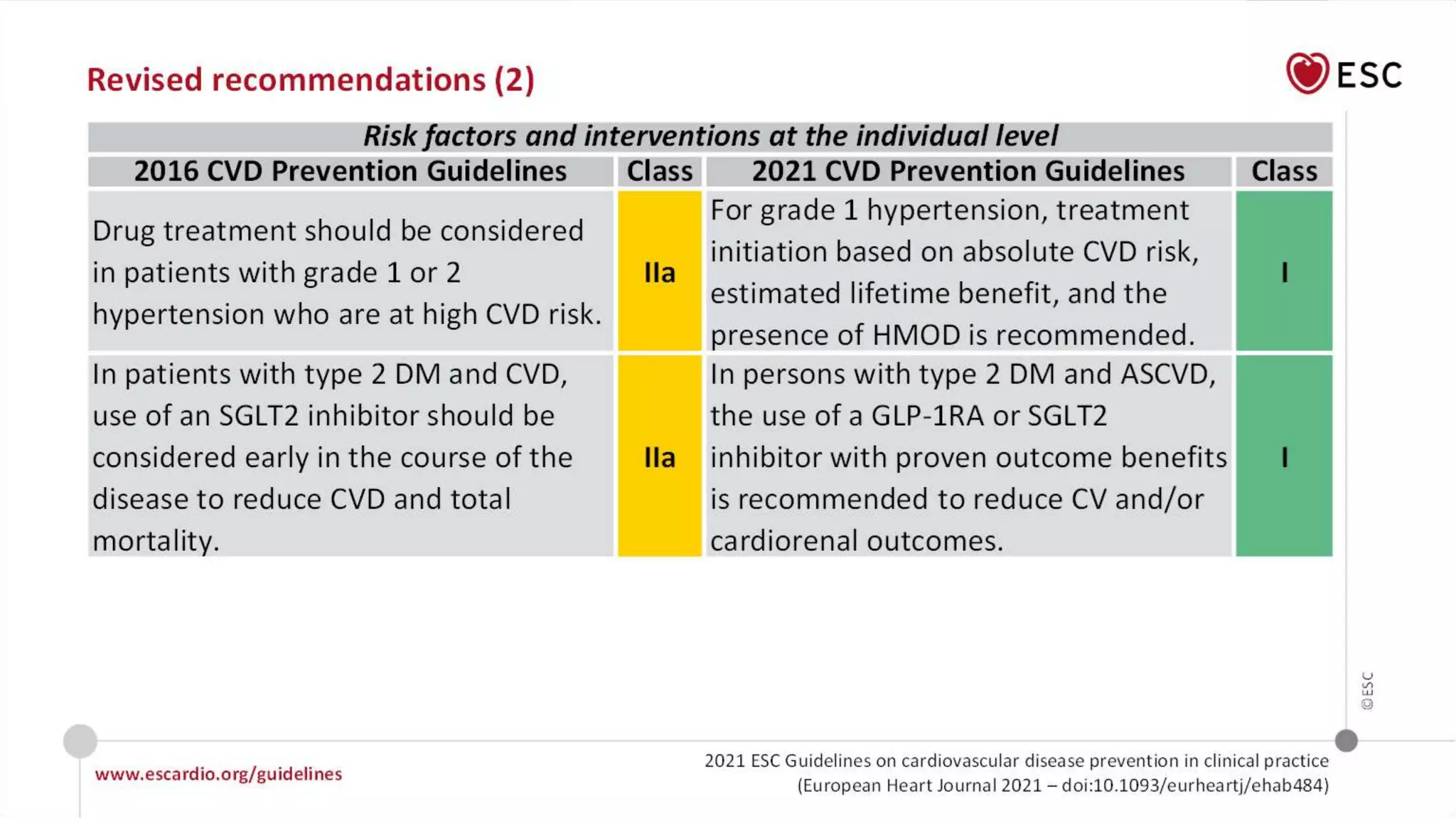
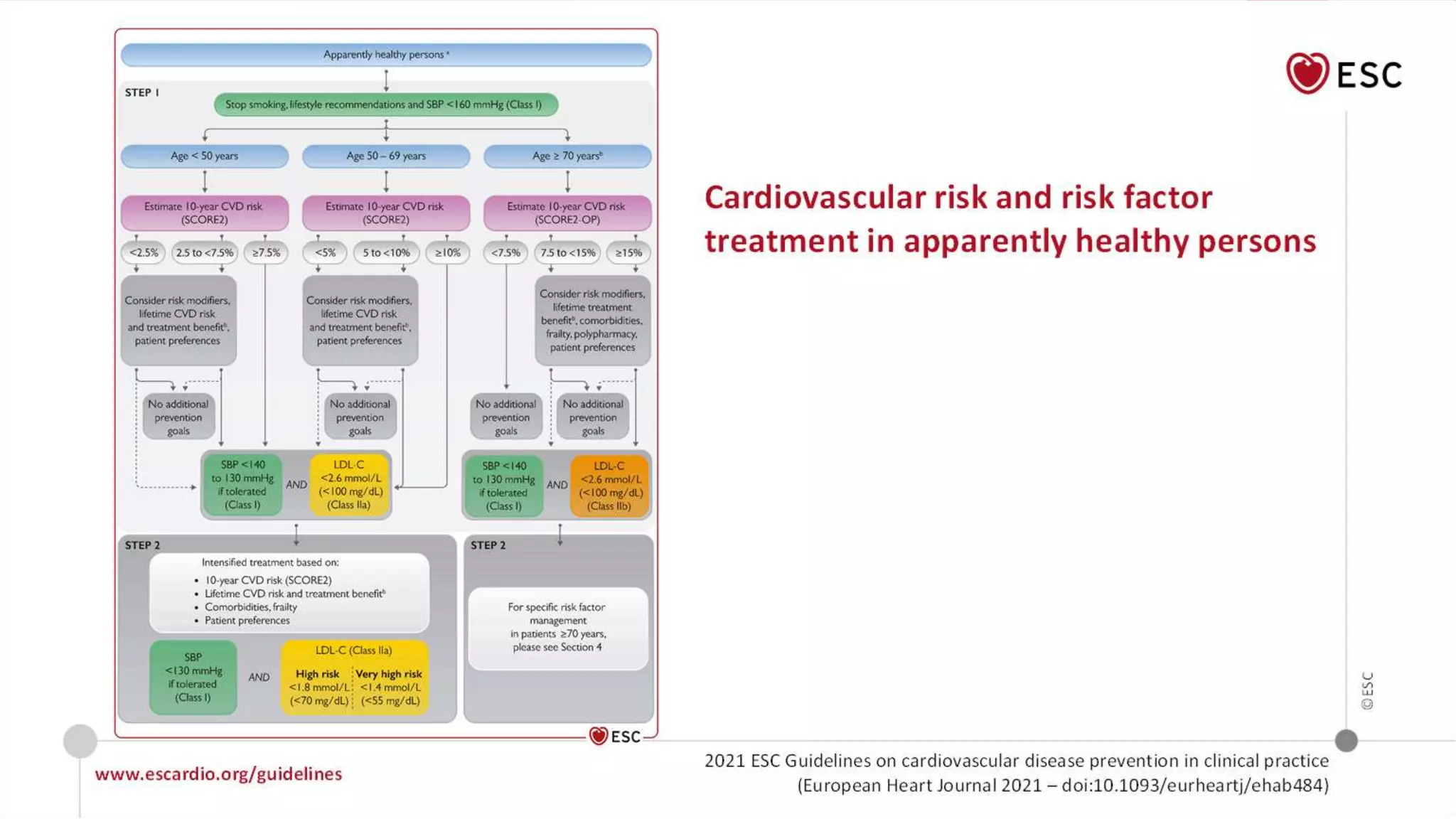
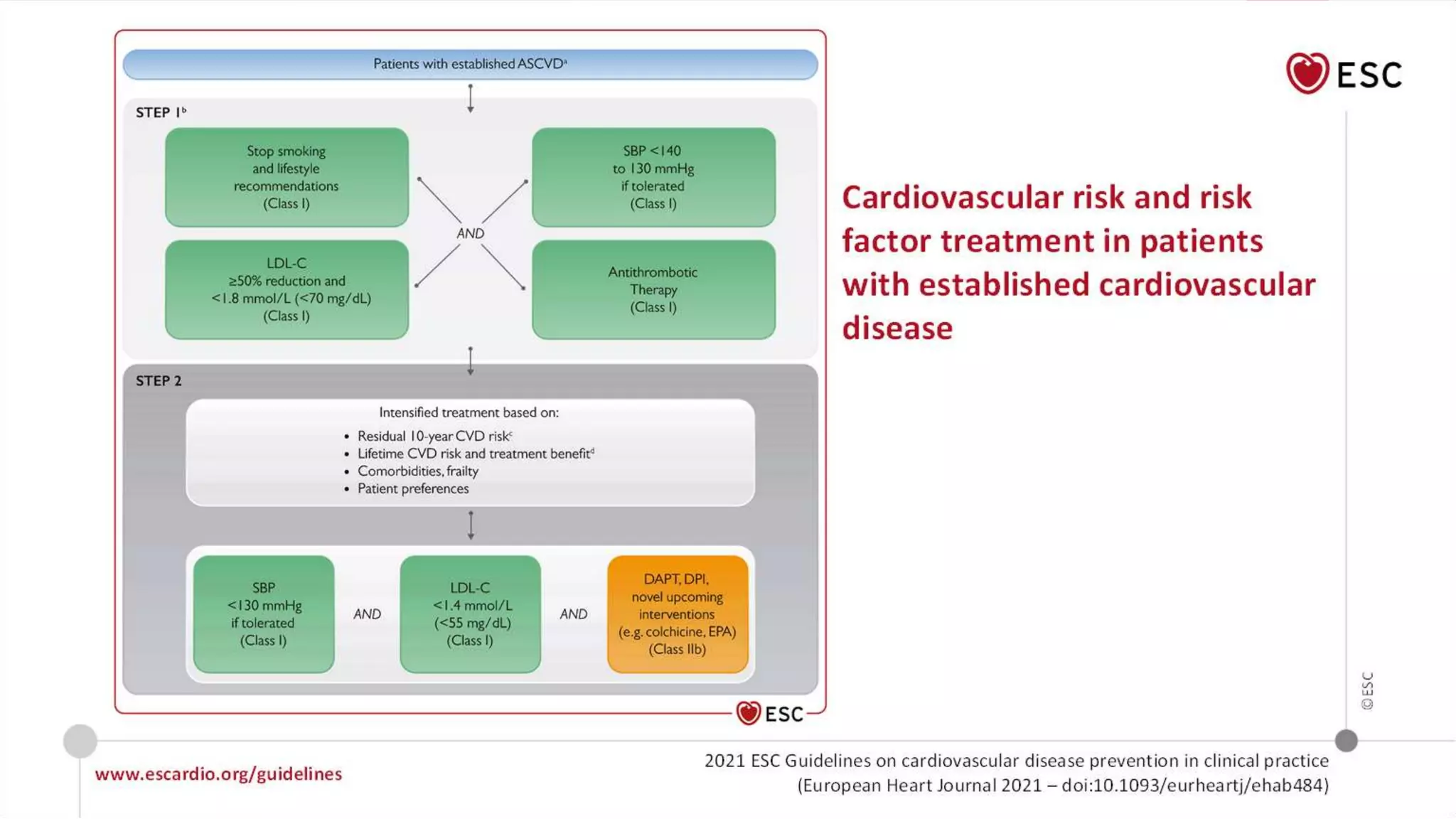
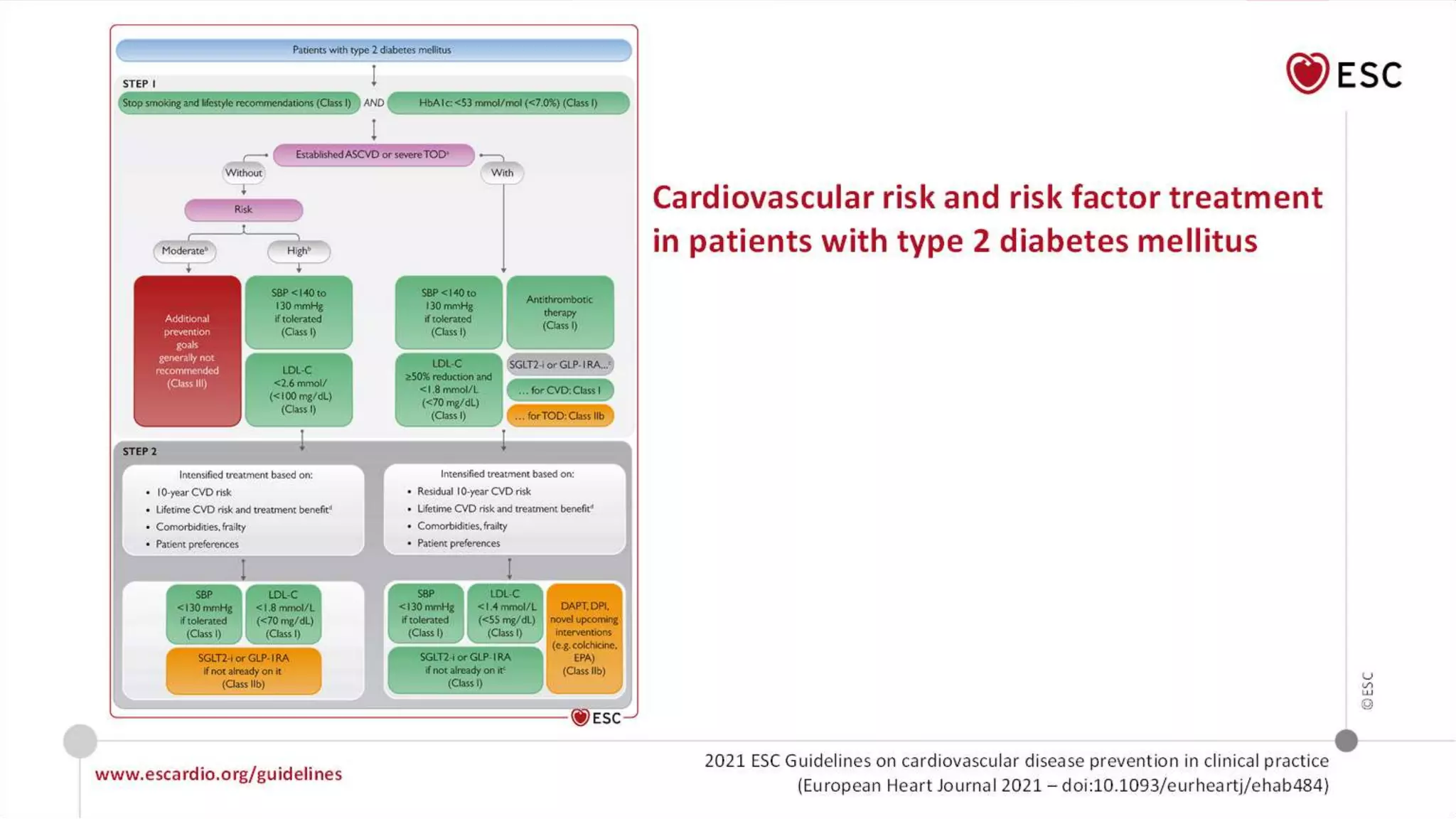
The document summarizes new recommendations from the 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. It provides recommendations on risk assessment tools, lifestyle interventions, pharmacological treatments, and management of specific cardiovascular diseases. The key recommendations include using SCORE2 to assess CVD risk, adopting a Mediterranean diet, treating risk factors according to guideline recommended targets, and enrolling patients with heart failure in cardiac rehabilitation programs.