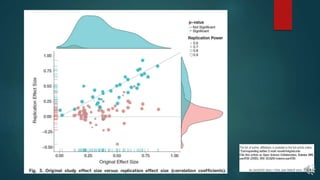
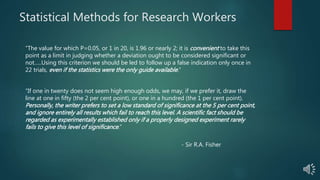
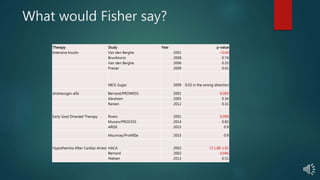
This document discusses several epistemic problems in critical care medicine related to evidence and knowledge. It outlines how the statement "there is evidence for" can obscure a more complex reality. Trials can produce false positives or negatives, and high prior probabilities of the null hypothesis combined with an alpha of 0.05 can lead to many false positive findings. It also discusses how problems like inadequate power from underestimated sample sizes and overestimated treatment effects can undermine trials and produce false negatives. Overall, the document advocates for more rigorous and nuanced interpretations of evidence that consider factors like prior probabilities, replication rates, and the limitations of statistical methods and trial designs.

![Knowledge without Formal Evidence
ARR high [NNT low]
“Visible” & immediate effects
Causal Pathways “Obvious”
Type I diabetes DKA
Insulin Resolution of DKA
Trials “unethical” – No Equipoise – High Prior Probability for
Ha
Implicit Bayesian Approach
Category 1 Therapies (Parachute Therapies)](https://image.slidesharecdn.com/epistemicproblems121815-151220051721/85/Epistemic-problems-12_18_15-6-320.jpg)
![No knowledge without Formal Evidence
Category 2 Therapies
ARR low(er) [NNT high(er)]
“Invisible” & delayed effects
Associations Prevalent, CPs Obscure
ICU Hyperglycemia ???
Insulin correction of hyperglycemia
Trials imperative – Equipoise - Low(er) Prior Probability for
Ha](https://image.slidesharecdn.com/epistemicproblems121815-151220051721/85/Epistemic-problems-12_18_15-8-320.jpg)