CONTENTS
1. Introduction
2. Definition
3.History
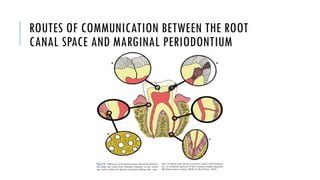
4. Routes of communication between the pulp and the
periodontium
5. Etiological factors
6. Classification
7. Diagnosis
8. Types of Endodontic-Periodontic lesion
9. Prosthetic considerations in management of endo-perio lesion
10. VRF as an endodontic-periodontic lesion
3.
PERIODONTAL MANAGEMENT
1. Gingivalcurettage
2. Flap surgery
3. Types of sutures
4. Osseous surgery
5. Management of furcation defects
Root resection
Hemisection
6. Periodontal reconstructive surgery
7. Local drug delivery systems
4.
INTRODUCTION
Understanding the interrelationshipbetween endodontic and periodontal diseases is
crucial for correct diagnosis, prognosis, and treatment decision making.
The dental pulp and the periodontium are closely related, and pathways of
communication between these structures often determine the progress of the disease
in these tissues.
5.
DEFINITION
An endo periolesion is defined as:
i.The tooth involved must be pulpless
ii.There must be destruction of the periodontal attachment apparatus from the
gingival sulcus to either the apex of the tooth or to the area of an involved lateral
canal ie there must be a defect that can be probed
iii.Both RCT and periodontal therapy are required to resolve the entirety of the lesion.
PRINCIPLES AND PRACTICE OF ENDODONTICS 3RD
EDITION- Walter and Torabinejad
6.
HISTORY
•In 1927 Cahndescribed the association of the degenerative changes in the pulp
tissues and periodontal disease.
•In 1972 Weine suggested that endodontics is actually “periapical periodontics.”
However, this term has not been widely accepted, like many others’ proposed
definitions
•In 1964 Simring and Goldberg put forward the first publication on this topic,
claiming that pulpal and periodontal problems are responsible for more than 50%
of tooth mortality.
1. DENTINAL TUBULES
•Directcommunication between the pulp and the periodontium may occur via patent
dentinal tubules if the cementum layer is interrupted.
•Dentinal exposure can be related to developmental defects, disease processes,or
surgical procedures involving root surfaces
•Radicular dentin tubules extending from the pulp to the cemento-dentinal junction run
a relatively straight course.
•Diameter of dentinal tubule
- at periphery-1µm
- towards pulp- 3µm
9.
•The density ofdentinal tubules
- At the cervical portion of root- 15,000/mm2
- Near the apex- 8,000/mm2
- Towards pulpal end- 57,000/mm2
•When the cementum and enamel do not meet at the cemento-enamel junction (CEJ)
tubules remain exposed, thus creating pathways of communication between the
pulp and the periodontal ligament.
10.
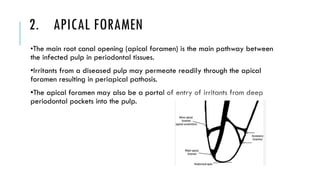
2. APICAL FORAMEN
•Themain root canal opening (apical foramen) is the main pathway between
the infected pulp in periodontal tissues.
•Irritants from a diseased pulp may permeate readily through the apical
foramen resulting in periapical pathosis.
•The apical foramen may also be a portal of entry of irritants from deep
periodontal pockets into the pulp.
11.
3. LATERAL ANDACCESSORY CANALS
•It is estimated that 30 to 40% of all teeth have lateral or accessory canals, mostly
found in the apical third of the root.
•De Deus12 found that 17% of the teeth examined presented lateral canals in the
apical third of the root, about 9% in the middle third, and less than 2% in the coronal
third.
•Accessory canals in the furcation of molars may also be pathways of communication
between the pulp and periodontium.
12.
•The reported incidenceof furcal accessory canals varies from 23 to
76%
•Seltzer et al suggested that patent accessory canals are a potential
pathway for the spread of microorganisms and their toxic byproducts,
as well as other irritants, from the pulp to the periodontal ligament and
vice versa, resulting in an inflammatory process in the involved tissues
`
INGLE’S ENDODONTICS 6TH EDITION
13.
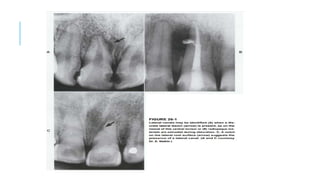
•Several clinical aids,however, may be helpful for their identification:
(1) a radiographic image of a discrete lateral lesion associated with a necrotic pulp;
(2) radiographic identification of a ‘‘notch’’ on the lateral root surface suggesting the
presence of an orifice; and
(3) demonstration of root canal filling material, or sealer, extruding through the patent
orifices.
MICROBIOLOGICAL FACTORS
•Zehnder etal. claimed that although the periodontal pocket presents a
greater variety of microorganisms than the infected pulp, when an endodontic
infection is caused by severe periodontitis, all bacterial species found within
the root canals are also present in the periodontal pocket.
•These similarities in the microflora of these two niches were also reported by
Kerekes and Olsen, supporting the concept that infection may spread from one
niche to the other.
17.
Spirochetes areassociated
with both endodontic and
periodontal diseases.
Spirochetes are found more
frequently in subgingival
plaque than in root canals.
The spirochete species most
frequently found in root canals
are Treponema denticola and
Treponema maltophilium.
•Rôças et al. assessed the
occurrence of the so-called
“red complex bacteria”
(Porphyromonas gingivalis,
Bacteroides forsythus, and
Treponema denticola) that
may be associated with
severe periodontal
diseases, in root canal
infections.
L-form bacteria may
also have a role in
endodontic disease, the
L-forms revert to their
original pathogenic
bacterial form and may
then be responsible for
acute exacerbation of
chronic apical lesions.
18.
2. FUNGI
• •The majority of these fungi are Candida albicans.
• • Fungi may also colonize canal walls and invade dentinal
tubules.
• • Other species such as Candida glabrata, Candida
guillermondii, Candida incospicia, and Rodotorula mucilaginosa
have also been detected.
• • It has also been demonstrated that the presence of fungi
in root canals is directly associated with their presence in saliva.
19.
3. VIRUS
In patientswith periodontal disease, herpes simplex virus was frequently
detected in gingival crevicular fluid gingival biopsies of periodontal lesions
• Human cytomegalovirus was observed in about 65% of
periodontal pocket samples and in about 85% of gingival tissue samples.
• • Epstein–Barr virus type I was observed in more than 40% of
pocket samples and in about 80% of the gingival tissue samples
• • Gingival herpes viruses were found to be associated with
increased occurrence of subgingival Porphyromonas gingivalis,
Bacteroides forsythus, Prevotella intermedia, Prevotella nigrescens, T.
denticola, and Actinobacillus actinomycetemcomitans, thus suggesting a
role in overgrowth of periodontal pathogenic bacteria.
20.
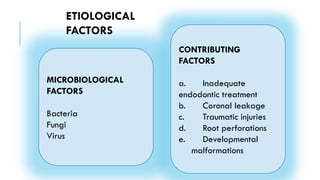
CONTRIBUTING FACTORS
a.INADEQUATE ENDODONTICTREATMENT
•It is essential to clean, shape, and obturate the canal system well in order to
enhance successful outcomes.
•Poor endodontic treatment often results in treatment failure.
21.
b. CORONAL LEAKAGE
•Defectiverestorations and adequate root canal fillings will have a higher
incidence of failures than teeth with inadequate root canal fillings and
adequate restorations.
•In an in vitro study, it was found that packing excess guttapercha and sealer
over the floor of the pulp chamber, after completion of root canal filling, did
not provide a better seal of the root canals.
•It is therefore recommended that excess of gutta-percha filling should be
removed to the level of the canal orifices and the floor of the pulp chamber
be protected with a well-sealed restorative material.
22.
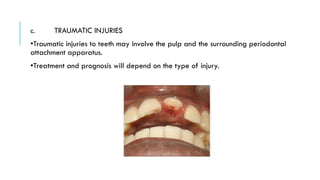
c. TRAUMATIC INJURIES
•Traumaticinjuries to teeth may involve the pulp and the surrounding periodontal
attachment apparatus.
•Treatment and prognosis will depend on the type of injury.
23.
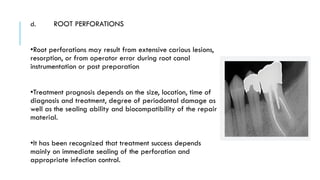
d. ROOT PERFORATIONS
•Rootperforations may result from extensive carious lesions,
resorption, or from operator error during root canal
instrumentation or post preparation
•Treatment prognosis depends on the size, location, time of
diagnosis and treatment, degree of periodontal damage as
well as the sealing ability and biocompatibility of the repair
material.
•It has been recognized that treatment success depends
mainly on immediate sealing of the perforation and
appropriate infection control.
24.
•Mineral Trioxide Aggregateis widely used to seal root perforations.
•Another treatment modality for perforations, root resorptions, and certain root
fractures in the cervical third region is orthodontic root extrusion.
•The procedure has a very good prognosis and a low risk of relapse. It can be
performed either immediately or over a few weeks period depending on each
individual case.
The goal of controlled root extrusion is to modify the soft tissues and bone and is
therefore used to correct gingival discrepancies and osseous defects of periodontally
involved teeth.
25.
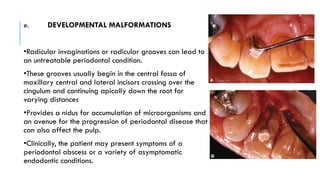
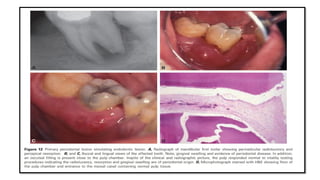
e. DEVELOPMENTAL MALFORMATIONS
•Radicularinvaginations or radicular grooves can lead to
an untreatable periodontal condition.
•These grooves usually begin in the central fossa of
maxillary central and lateral incisors crossing over the
cingulum and continuing apically down the root for
varying distances
•Provides a nidus for accumulation of microorganisms and
an avenue for the progression of periodontal disease that
can also affect the pulp.
•Clinically, the patient may present symptoms of a
periodontal abscess or a variety of asymptomatic
endodontic conditions.
26.
•It can bediagnosed by visually by probing tubular depth.
•The tooth will also respond to pulp testing procedures
•The prognosis of root canal treatment in such cases is guarded, depending on the
apical extent of the groove
•Treatment consists of burring out the groove, placing bone substitutes, and surgical
management of the soft tissues and underlying bone.
• A clinical case using Emdogain as a treatment adjunct was recently described
27.
CLASSIFICATION OF ENDODONTIC-
PERIODONTALLESIONS
Classification 1
Simon et al. in 1972 were the first to suggest a classification of
endodontic-periodontal lesions that was mainly based on diagnosis,
prognosis, and treatment.
i. primary endodontic lesions,
ii. primary periodontal lesions,
iii.primary endodontic lesions with secondary periodontal involvement,
iv. primary periodontal lesions with secondary endodontic involvement
v. true combined lesion
28.
Classification 2
Torabinejadand Trope in 1996, based on the origin of the periodontal
pocket:
i. endodontic origin,
ii. periodontal origin,
iii.combined endo-perio lesion,
iv. separate endodontic and periodontal lesions,
v. lesions with communication,
vi.lesions with no communication
29.
Classification 3
Classificationwas recommended by the world workshop for
classification of periodontal diseases (1999), Periodontitis
Associated with Endodontic Disease:
i. endodontic-periodontal lesion,
ii. periodontal-endodontic lesion,
iii.combined lesion.
30.
Classification 4
Anew endodontic-periodontal interrelationship classification, based on the
primary disease with its secondary effect, is suggested as follows:
i. retrograde periodontal disease:
a. primary endodontic lesion with drainage through the periodontal ligament,
b. primary endodontic lesion with secondary periodontal involvement;
i. primary periodontal lesion;
ii. primary periodontal lesion with secondary endodontic involvement;
iii.combined endodontic-periodontal lesion;
iatrogenic periodontal lesions
31.
DIAGNOSIS
MEDICAL HISTORY
Theage of the patient and current medical conditions can influence both the
diagnosis and course of treatment.
Patients with diabetes mellitus have been associated with increased risk to
periodontal disease and may also be at greater risk of developing apical
periodontitis
Recent evidence has also been presented suggesting patients with periodontal
disease may have delayed healing after endodontic therapy.
Many patients being treated for cardiovascular disease also have
hypercholesterolemia and are most likely taking a statin drug. As a result, they
may be at risk of developing pulp canal obliteration over time, which may
make the tooth more susceptible to developing apical periodontitis.
32.
DENTAL HISTORY
Questionnaireon the type, character , diurnal variation of pain.
These questions are designed to determine the nature of the problem, as
endodontic symptoms (history of spontaneous pain, lingering pain to cold, pain to biting) usually
develop over a period of weeks or months, but periodontal related symptoms (sore gums, bleeding
gums, foul odor) may linger for months to years.
Another important question to consider pertains to the possibility of a history of trauma
Another important question to ask as part of the dental history involves previous endodontic
treatments
Ruiz et al. has shown that the risk of developing apical periodontitis in endodontically treated teeth is
5.19 times greater for patients with periodontal disease compared to patients without the disease
33.
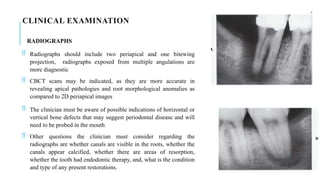
CLINICAL EXAMINATION
RADIOGRAPHS
Radiographsshould include two periapical and one bitewing
projection, radiographs exposed from multiple angulations are
more diagnostic
CBCT scans may be indicated, as they are more accurate in
revealing apical pathologies and root morphological anomalies as
compared to 2D periapical images
The clinician must be aware of possible indications of horizontal or
vertical bone defects that may suggest periodontal disease and will
need to be probed in the mouth
Other questions the clinician must consider regarding the
radiographs are whether canals are visible in the roots, whether the
canals appear calcified, whether there are areas of resorption,
whether the tooth had endodontic therapy, and, what is the condition
and type of any present restorations.
34.
INTRAORAL EXAMINATION
Periodontalprobing, palpation, percussion, and sensibility testing (Cold test and Electric Pulp Test (EPT)) of
the suspected area will all need to be carefully considered.
35.
PERIODONTAL PROBING
Agingival abscess of periodontal origin would commonly have wide areas of
pocketing compared to those from an endodontic origin, which tend to be
narrower.
A fine periodontal probe must be used (Marquis periodontal probe, Marquis
Dental Manufacturing Co., Denver, CO).
36.
PERCUSSION
It isimportant to discern whether the percussion sensitivity is coming from
an inflamed periodontal ligament (PDL), or is it from dentinal sensitivity
due to caries or a cuspal fracture.
Percussion sensitivity that is present no matter where the tooth is tapped
(buccal, occlusal, or lingual) is most probably from an inflamed PDL and
apical periodontitis.
Isolated areas of percussion sensitivity on the same tooth suggest a dentinal
issue, such as a fracture, caries, or possible occlusal trauma.
Endodontic etiologies tend to be more percussion sensitive than periodontal
ones
37.
SENSIBILITY TESTING
Resultsof sensibility tests are a critical element in determining whether the
diseased condition of the tooth is periodontal or endodontic origin.
An etiology of endodontic origin is easily ruled out if the offending tooth
responds normally to those tests
39.
PRIMARY ENDODONTIC DISEASE
A deep solitary pocket in the absence of periodontal disease may indicate
the presence of a lesion of endodontic origin.
For diagnosis purposes, a gutta-percha cone, or another tracking
instrument, should be inserted into the sinus tract and radiographs taken.
This will determine the origin of the lesion.
A sulcular pocket of endodontic origin is typically very narrow compared
to a pocket of periodontal origin. A similar condition occurs where drainage
from the apex of a molar extends coronally into the furcation area
40.
Primary endodonticlesions usually heal following root canal treatment.
The sinus tract extending into the gingival sulcus or furcation area quickly
heals once the affected pulp has been removed and the root canals cleaned,
shaped, and obturated
According to Whyman et al,Surgical endodontic therapy has been shown
to be unnecessary even in the presence of large periradicular radiolucencies
and periodontal abscesses
43.
PRIMARY PERIODONTAL DISEASE
These types of conditions are caused primarily by periodontal pathogens.
In this process, chronic marginal periodontitis progresses apically along
the root surface.
In most cases, pulp tests indicate a clinically normal pulpal reaction
There is frequently an accumulation of plaque and calculus and the pockets
are wider.
The prognosis depends upon the stage of periodontal disease and the
efficacy of periodontal treatment.
44.
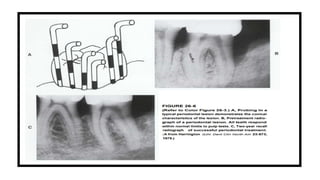
In periodontaldisease bone loss always begins at crestal bone level and progresses
apically.
The typical lesion is conical in contour. The probing may start from a sulcus depth that
is within normal limits, then gradually step down a slope to the apical extent of the
lesion, and then step up again on the other side to a sulcus depth within normal limits.
The slope of the lesion will vary and may depend on the coronal width of the lesion.
Regardless of the degree of the slope, a distinctive conical shape will be distinguished
by carefully feeling the increasing and then de-creasing depth of the attachment as the
periodontal probe is stepped down into and then up out of the lesion
45.
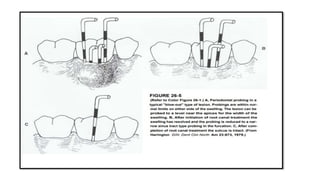
Occasionally theclinical presentation of a periodontal lesion will have the
sloping contour of a conical lesion on one side but a more precipitous,
sharp drop-off on the other. Such probing should be considered to be of the
"periodontal type" of probing.
A periodontal lesion will not resolve in response to root canal treatment
even if the associated tooth is pulpless. The prognosis for a tooth with
conical shaped probing must be based on the prognosis for resolving the
periodontal lesion.
If it can be demonstrated that a tooth is pulpless and if the periodontal
prognosis is favorable, root canal treatment should be completed before
periodontal therapy. In summary, conical shaped probing indicates
periodontal pathosis
46.
Primary periodontallesions are treated by hygiene phase therapy in the first
instance. Subsequently, poor restorations and developmental grooves that are
involved in the lesion are removed as these are difficult areas to treat successfully.
Periodontal surgery is performed after the completion of hygiene phase therapy if
deemed necessary
49.
PRIMARY ENDODONTIC DISEASEWITH
SECONDARY PERIODONTAL INVOLVEMENT
Untreated suppurating primary endodontic disease may sometimes become secondarily
involved with marginal periodontal breakdown.
In such cases, marginal periodontitis is developed as a result of plaque formation at the
gingival margin of the sinus tract.
When plaque or calculus is present, the treatment and prognosis of the tooth are
different than those of teeth involved with only primary endodontic disease.
The tooth now requires both endodontic and periodontal treatments. If the endodontic
treatment is adequate, the prognosis depends on the severity of the marginal periodontal
damage and the efficacy of periodontal treatment. With endodontic treatment alone, only
part of the lesion will heal to the level of the secondary periodontal lesion
50.
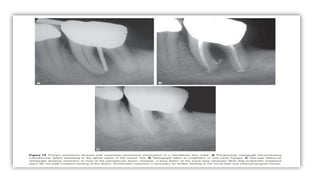
A similarclinical picture may also occur as a result of root perforation
during root canal treatment, or where pins or posts have been misplaced
during coronal restoration.
Sometimes, symptoms may be acute, with periodontal abscess formation
associated with pain, swelling, purulent exudate, and pocket formation and
tooth mobility
Root fractures may also mimic the appearance of primary endodontic
lesions with secondary periodontal involvement.
These typically occur on endodontically treated teeth often with a large
post. In such cases, a local deepening of a periodontal pocket and more
acute periodontal abscess symptoms can be found
52.
PRIMARY PERIODONTAL DISEASEWITH
SECONDARY ENDODONTIC INVOLVEMENT
A periodontal pocket may continue and progress until the apical tissues are
involved. In this case, the pulp may become infected due to irritants entering via
lateral canals or the apical foramen and subsequently become necrotic.
In single-rooted teeth, the prognosis is usually poor. In molar teeth, the
prognosis may be better because not all the roots may suffer the same loss of
supporting tissues.
In some of these cases, root resection can be considered as a treatment alternative
Bacteria originating from the periodontal pocket can be a source of root canal
infection.
53.
A strongcorrelation between the presence of microorganisms in root canals
and their presence in periodontal pockets of advanced periodontitis has
been demonstrated indicating that similar pathogens may be involved in
both diseases
Treatment complications of periodontal disease can also lead to secondary
endodontic involvement. Lateral canals and dentinal tubules may be opened
to the oral environment by curettage, scaling, or surgical flap procedures. In
such cases, blood vessels within a lateral canal can be severed by a curette
and microorganisms introduced into the area during treatment
55.
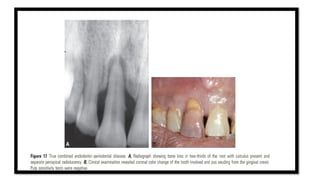
TRUE COMBINED DISEASES
True combined diseases occur less often. They are usually formed when an endodontic
disease progressing coronally joins with an infected periodontal pocket progressing
apically
The degree of attachment loss in this type of lesions is large and the prognosis guarded
in single-rooted teeth
In most cases, periapical healing may be anticipated following successful endodontic
treatment. However, the periodontal tissues may not respond well to treatment, and
healing will depend on the severity of the condition
The radiographic appearance of combined endodontic-periodontal disease may be
similar to that of a vertically fractured tooth.
56.
A fracturethat has invaded the pulp space causing pulp necrosis may also
be considered a true combined lesion and yet not be amenable to successful
treatment.
Often, it is necessary to perform surgical exploration of the affected site to
confirm the diagnosis
True-combined lesions are treated initially as primary endodontic lesions
with secondary periodontal involvement. The prognosis of a true-combined
perio-endo lesion is often poor or even hopeless, especially when
periodontal lesions are chronic with extensive loss of attachment.
57.
Root amputation,hemisection or separation may allow the root
configuration to be changed sufficiently for part of the root structure to be
saved
The prognosis of an affected tooth can also be improved by increasing bony
support which can be achieved by bone grafting and guided tissue
regeneration. This is due to the most critical determinant of prognosis being
a loss of periodontal support
59.
ACUTE OR "BLOW-OUT"LESIONS
When a patient presents with a localized swelling that involves the gingival sulcus, it may
be difficult to determine if the swelling is due to a periodontal abscess or an abscess of
endodontic origin.
The swelling is usually on the labial or buccal side of the tooth but may be on the lingual
side.
As the sulcus is probed there is usually normal sulcus depth all the way around the tooth
until the area of the swelling is probed
At the edge of the swelling the probe drops precipitously to a level near the apex of the
tooth, and the probing depth remains the full width of the swelling
This swelling can be characterized as having "blown out" the entire attachment on that side
60.
When probingcarefully around the neck of the tooth in the area of swelling,
intact crestal bone
This would indicate that there has been a pathologic perforation of the cortical
plate farther apically and that the periosteum has been lifted off the coronal
cortical plate by the swelling.
If intact crestal bone is present, rapid reattachment can be expected after
resolution of the swelling. In some instances, on the other hand, careful
probing will reveal the absence of the buccal cortical plate to the depth of
approximately the apical extent of the swelling.
With this blow out type of probing, indicating loss of bone along a broad front,
rapid reattachment can also be expected. In furcations, however, healing may
first proceed to what will be described later in this chapter as a "sinus tract
type of probing," but eventually complete reattachment can be expected.
61.
Treatment fora blow out lesion involves customary endodontic emergency
procedures that would be used if there were a similar swelling but the entire
sulcus were intact. The root surface need not be curetted, nor the area
surgically flapped.
Endodontic treatment only is indicated. As the result of endodontic
management of the swelling, complete periodontal reattachment occurs
within 1 week in most cases.
However, the broad, precipitous probing may resolve to a narrow, deep
sinus tract type of probing, which may remain until after completion of root
canal treatment.
63.
PROSTHETIC CONSIDERATIONS INTHE MANAGEMENT
OF ENDODONTIC PERIODONTAL LESIONS
Restoration of endo-perio treated teeth can be challenging due to their doubtful
prognosis.
Direct restoration involves placement of a restorative material (amalgam or composite)
into the tooth while Indirect restorations consist of cast metal or ceramic crowns or
indirect partial restorations (e.g., inlays and onlays)
Loss of tooth structure greater than 50%, especially marginal ridges loss, would
determine the use of root posts to retain a core
The preservation of sound root structure while using posts increases fracture resistance
and decreases occurrence of periapical lesions of the restored endo-perio treated teeth
64.
Posts witha reduced length in combination with composite resin cement
are recommended in order to improve tooth survival
Based on the evidence, root filled posterior teeth with limited coronal loss,
where 50% or more coronal structure is preserved, can be restored without
intraradicular retention, predominantly when indirect or indirect partial
restorations are used
Coronal leakage is considered a major factor that influences tooth survival
during and after canal treatment due to bacteria and endotoxin penetration
along the root canal filling
65.
A highersuccess rate was found in treated teeth with permanent
restorations vs. provisional restorations, the study recommended a proper
and prompt permanent restoration after completion of endodontic treatment
Resin cements are recommended as efficient coronal sealers due to
minimizing micro leakage potential for both posts and indirect restorations,
by creating adhesion to the tooth substance.
A ferrule is highly desirable when indirect restoration is used. A suitable
ferrule is considered a minimum of 2 mm of vertical height and 1 mm of
dentin thickness.
66.
VRF AS ANENDODONTIC PERIODONTAL LESION
Vertical root fracture (VRF) is a root canal treatment complication and
probably the third reason for extraction of endodontically treated teeth
According to the AAE consensus statement, the combination of sinus tract
and deep isolated probing defect in the endodontically treated tooth is
pathognomonic for this entity
It was shown, in 2010 by Tsesis et al, that there is no substantive evidence-
based data concerning the diagnostic accuracy as to the effectiveness of
clinical and radiographic evaluation of VRF diagnosis.
67.
Vertical rootfractures are chronic longitudinally oriented fractures, with an
apicocoronal direction.
Study regarding reasons for extraction of endodontically treated teeth
showed that the vertically fractured teeth amount to 11% of the extracted
teeth
VRFs can originate at any level along the root although it appears that they
usually initiate at the apical part. If they originate in the middle part of the
root, they can propagate in either direction, apical or coronal
68.
Rarely doesa VRF have a mesio-distal orientation
Patient’s signs and symptoms of VRFs are similar to those of periodontal
disease or failing endodontic treatment.
In addition, they are usually diagnosed years after the endodontic and
prosthodontic procedures have been completed.
The periodontal destruction resulting from the communication of the root
canal space with the periodontium and its contamination is a slow process
An isolated deep probing pocket, sometimes all the way to the root apex
practically facing the fracture line, is considered typical clinical sign for the
bone loss in the vertically fractured root
69.
In the“true” periodontal cases, the pocket is initiated most of the time in
the interproximal areas and the bone resorption is initiated in the crestal
area.
When the isolated bony defect in the suspected VRF tooth does exists, it is
not easy sometimes to probe the pocket and patient discomfort can also be
an issue
To achieve the accurate VRF diagnosis, the probing finding should be
coupled with other signs such as a sinus tract .
In VRF cases, the sinus tract is usually highly located in the attached
gingiva as compared to a chronic apical abscess from a failing
endodontically treated tooth
70.
The teethand roots most susceptible to VRF are those in which their mesio-
distal diameter in cross section is narrow compared to the buccolingual
dimension (oval, hourglass shaped, kidney shaped, ribbon shaped).
Such teeth and roots are the maxillary and mandibular premolars, the
mesial root of mandibular molars, the mandibular anterior teeth, and mesio-
buccal roots of the maxillary molars
One of the most frequent bony radiolucencies seen around VRF teeth
radiographic feature of VRF is the “halo” (“J shaped”) appearance.
71.
This isa combined periapical and lateral radiolucency along the side of the
root, or a lateral radiolucency on one or both sides of the root. Another
typical bony radiolucency is the “angular” type. It is an angular
radiolucency from the crestal bone terminating on the side of the root
The “angular” radiolucency is more often typical in a case with a “true”
periodontal disease, but as in the previous more “typical” bony
radiolucencies of a VRF tooth, it is only the presence of the
“pathognomonic combination” of clinical signs and symptoms that will
confirm the diagnosis
72.
Lustig etal. found that in most patients with other signs and symptoms
(sinus tract, large osseous defect, mobility) or with acute exacerbations,
greater interproximal bone loss was recorded than in patients in whom the
VRF diagnosis was made at an early stage of the coronal third
However in the last consensus statement by the AAE it was stated that in
the majority of cases the indication of a VRF is often due to the specific
pattern of bone loss and PDL space enlargement rather than direct
visualization of the fracture
REFERENCES
1. INGLE’S ENDODONTICS6TH
, 7TH
EDITION
2. COHENS PATWAYS OF PULP12TH EDITION
3. ENDODONTIC PERIODONTIC LESION-Igor Tsesis Carlos, E. Nemcovsky, Joseph Nissan, Eyal
Rosen
4. PRINCIPLES AND PRACTICE OF ENDODONTICS 3RD
EDITION- Walter and Torabinejad
5. CARRANZA’S CLINICAL PERIODONTOLOGY- 10th
EDITION- Michael G . Newman, Henry H.
Takei
6. ESSENTIAL OF CLINICAL PERIODONTOLOGY AND PERIODONTICS- Shantipriya Reddy
PERIODONTAL MANAGEMENT
1. Gingivalcurettage
2. Flap surgery
3. Types of sutures
4. Osseous surgery
5. Management of furcation defects
Root resection
Hemisection
6. Periodontal reconstructive surgery
7. Local drug delivery systems
8. Conclusion
9. References
77.
PERIODONTAL SURGERY CANBE DIVIDED INTO:
1. POCKET REDUCTION
SURGERY
Resective (gingivectomy, apically
displaced flap and undisplaced flap
with or without osseous resection)
Regenerative (flaps with grafts,
membranes, etc.)
2. CORRECTION OF
MORPHOLOGIC DEFECTS
Plastic surgery techniques to widen
attached gingiva(free gingival grafts,
and other techniques, etc.)
Esthetic surgery (root coverage,
recreation of gingival papillae)
Preprosthetic techniques (crown
lengthening, ridge augmentation,
vestibular deepening)
Placement of dental implants,
including techniques for site
development for implants (guided bone
regeneration, sinus grafts)
78.
OBJECTIVES OF THESURGICAL PHASE
Improvement of the prognosis of teeth and their
replacements
Improvement of esthetics.
79.
SURGICAL POCKET THERAPY
Pocket elimination consists of reducing the depth of periodontal pockets to
that of the physiologic sulcus to enable cleansing by the patient.
By proper case selection, both resective techniques and regenerative
techniques can be used to accomplish this goal.
81.
Pocket depthis an extremely useful and widely employed clinical determination,
but it must be evaluated together with level of attachment and the presence of
bleeding, exudation, and pain.
The most important variable for evaluating whether a pocket for deep sulcus is
progressive is the level of attachment, which is measured in millimeters from the
cementoenamel junction.
84.
INDICATIONS FOR PERIODONTALSURGERY
1. Areas with irregular bony contours, deep craters, and other defects usually require surgical
approach.
2. Pockets on teeth in which a complete removal of root irritants is not considered
clinically possible may call for surgery. This occurs frequently in molar and premolar areas
3. In cases of furcation involvement of grade 11 or III, a surgical approach ensures the removal
of irritants; any necessary root resection or hemisection also requires surgical intervention
4. Intrabony pockets on distal areas of last molars, frequently complicated by mucogingival
problems, are usually unresponsive to nonsurgical methods
5. Persistent inflammation in areas with moderate to deep pockets may require a surgical
approach. In areas with shallow pockets or normal sulci, persistent inflammation may point
to the presence of a mucogingival problem that needs a surgical solution
85.
Lindhe etal proposed guidelines for decision making based on critical
probing depth:
•Critical probing depth for scaling and root planning(SRP): 2.9mm
Below this critical PD of 2.9mm, if SRP is done, attachment loss occurs; when
PD> 2.9mm, SRP result in attachment gain
•Critical PD for modified Widman flap(MWF): 4.2mm
Below this critical PD of 4.2mm, if MWF surgery if done, attachment loss
occurs; when PD>4.2 mm MWF results in attachment gain
•MWF trumps SRP at 5.5mm
Pockets deeper than 5.5mm respond better to MWF than SRP with more gain
in attachment levels.
86.
GINGIVAL CURETTAGE
Theterm curettage is used in periodontics to mean the scraping of gingival
wall of a periodontal pocket to separate diseased soft tissue
The main accomplishment of curettage is the removal of chronically-
inflamed granulation tissue that forms in the lateral wall of the periodontal
pocket.
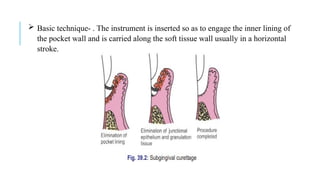
87.
Basic technique-. The instrument is inserted so as to engage the inner lining of
the pocket wall and is carried along the soft tissue wall usually in a horizontal
stroke.
88.
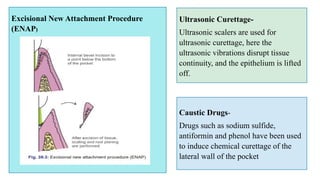
Excisional New AttachmentProcedure
(ENAP)
Caustic Drugs-
Drugs such as sodium sulfide,
antiformin and phenol have been used
to induce chemical curettage of the
lateral wall of the pocket.
Ultrasonic Curettage-
Ultrasonic scalers are used for
ultrasonic curettage, here the
ultrasonic vibrations disrupt tissue
continuity, and the epithelium is lifted
off.
89.
FLAP SURGERY
Definition-A periodontal flap is a section of gingiva and/or mucosa surgically-
elevated from the underlying tissues to provide visibility of and access to the bone
and root surface
Indication-
i. Gain access for root debridement.
ii. Reduction or elimination of pocket depth, so that patient can maintain the root
surfaces free of plaque.
iii.Reshaping soft and hard tissues to attain a harmonious topography (physiologic
architecture).
iv. Regeneration of alveolar bone, periodontal ligament and cementum
90.
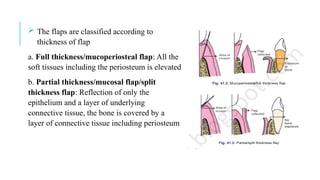
The flapsare classified according to
thickness of flap
a. Full thickness/mucoperiosteal flap: All the
soft tissues including the periosteum is elevated
b. Partial thickness/mucosal flap/split
thickness flap: Reflection of only the
epithelium and a layer of underlying
connective tissue, the bone is covered by a
layer of connective tissue including periosteum
91.
According tothe Placement of Flap after Surgery
a. Nondisplaced flap: The flap is returned and sutured back in its
original position.
b. Displaced flaps: The flap is repositioned coronal, apical or lateral to
its original position. However, palatal flaps cannot be displaced due to
the absence of unattached gingiva
92.
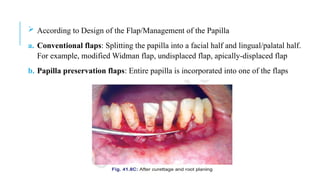
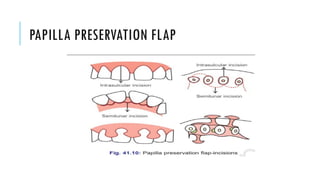
According toDesign of the Flap/Management of the Papilla
a. Conventional flaps: Splitting the papilla into a facial half and lingual/palatal half.
For example, modified Widman flap, undisplaced flap, apically-displaced flap
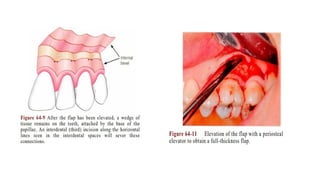
b. Papilla preservation flaps: Entire papilla is incorporated into one of the flaps
Flaps canbe reflected using only the horizontal incision if sufficient
access can be obtained in this way and if apical, lateral, or coronal
displacement of the flap is not anticipated.
If no vertical incisions are made, the flap is called an envelope flap.
98.
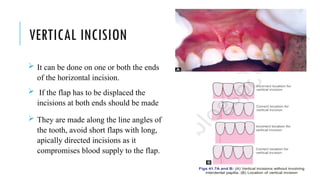
VERTICAL INCISION
Itcan be done on one or both the ends
of the horizontal incision.
If the flap has to be displaced the
incisions at both ends should be made
They are made along the line angles of
the tooth, avoid short flaps with long,
apically directed incisions as it
compromises blood supply to the flap.
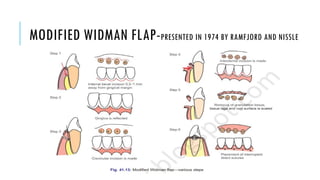
Step 1:The pockets are measured with the periodontal probe and a bleeding
point is produced on the outer surface of the gingiva to mark the base of the
pocket. In this procedure, the final placement of the flap is determined by first
incision
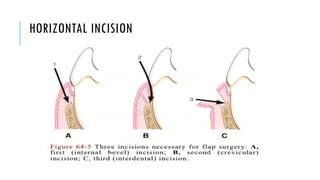
Step 2: The initial, internal bevel incision is made following the scalloping
bleeding points made on the gingiva. This incision is usually carried to a point
apical to the alveolar crest depending on the thickness of the tissue. The thicker
the tissue, the more apical will be the end point. The flap should be thinned with
the initial incision only.
Step 3: The second or crevicular incision is made from the bottom of the pocket
to the bone
Step 4: The flap is then reflected with a periosteal elevator (blunt dissection).
102.
Step 5:Interdental incision is made with an Orban’s interdental knife.
Step 6: Triangular wedge of tissue is removed with a curette
Step 7: The area is debrided, removing tissue tags and granulation tissue with sharp
curettes. The roots are scaled.
Step 8: The flap is then placed back to end at the root bone junction.
Step 9: The flaps are sutured together with continuous sling suture or interrupted
sutures.
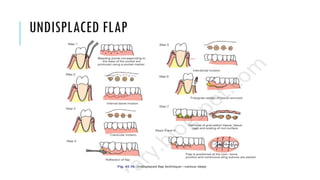
Step 1:The pockets are measured with the periodontal probe and a bleeding point
is produced on the outer surface of the gingiva to mark the base of the pocket. In
this procedure, the final placement of the flap is determined by first incision
Step 2: The initial, internal bevel incision is made following the scalloping
bleeding points made on the gingiva. This incision is usually carried to a point
apical to the alveolar crest depending on the thickness of the tissue. The thicker
the tissue, the more apical will be the end point. The flap should be thinned with
the initial incision only
Step 3: The second or crevicular incision is made from the bottom of the pocket to
the bone.
105.
Step 4:The flap is then reflected with a periosteal elevator (blunt
dissection).
Step 5: Interdental incision is made with an Orban’s interdental knife
Step 6: Triangular wedge of tissue is removed with a curette.
Step 7: The area is debrided, removing tissue tags and granulation tissue
with sharp curettes.
Step 8: The flap is then placed back to end at the root bone junction
106.
TYPES OF SUTURES
Thepurpose of suturing is to maintain the flap in the desired position until healing
has progressed to the point where sutures are no longer needed without tension
TECHNIQUE OF SUTURING
i. The needle is held with the needle holder and should enter the tissues at right
angles and no less than 2 to 3 mm from the incision.
ii. The needle is then carried through the tissue, following the needle's curvature.
iii. The knot should not be placed over the incision.
iv. The periodontal flap is closed either with independent sutures or with
continuous, independent sling sutures
107.
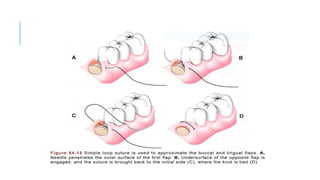
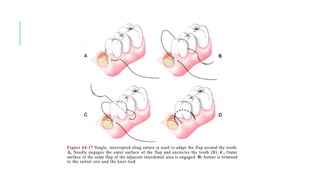
v.The latter methodeliminates the pulling of the buccal and lingual or palatal flaps
together and instead uses the teeth as an anchor to the flaps.
vi.The flaps are less likely to buckle, and the forces on the flaps are better
distributed.
vii.Sutures of any type placed in the interdental papillae should enter and exit the
tissue at a point located below the imaginary line that forms the base of the triangle
of the interdental papilla .
111.
OSSEOUS SURGERY
Definition: Osseous surgery may be defined as the procedure by which changes
in the alveolar bone can be accomplished to rid it of deformities induced by the
periodontal disease process or other related factors, such as exostosis and tooth
supraeruption
Osteoplasty—It is defined as reshaping of the alveolar process to achieve a more
physiologic form without removal of supporting bones.
Ostectomy—It is defined as the excision of bone or portion of a bone in
periodontics, removes supporting bone
112.
Horizontal BoneLoss= It is the most common pattern of bone loss in
periodontal disease. The bone is reduced in height but the bone margins
remain roughly perpendicular to the tooth surface
Vertical or Angular Defects =They are those that occur in an oblique
direction, leaving a hollowed out trough in the bone alongside the root, the
base of the defect is located apical to the surrounding bone
113.
Angular defects areclassified on the basis of number of walls present as:
One-walled or hemiseptal defect—One wall is present
Two-walled defect—Two walls are present
Three-walled or intrabony defect—Three walls are present (more common
on mesial surfaces of upper and lower molars)
Combined osseous defect—The number of walls in the apical portion of
the defect are greater than that in its occlusal portion.
115.
One-wall angulardefects usually need to be recontoured surgically.
Three-wall defects, particularly if they are narrow and deep, can he successfully
treated with techniques that strive for new attachment and bone reconstruction.
Two-wall angular detects can be treated with either method, depending on their depth,
width, and general configuration.
Therefore, except for one-wall defects and wide, shallow two-wall defects, along with
interdental craters, osseous defects are treated with the objective of obtaining optimal
repair by natural healing process
116.
TERMINOLOGIES
Graft: It isa viable tissue/organ that after removal from donor site is
implanted/transplanted within the host tissue, which is then repaired, restored
and remodelled.
Xenograft or heterograft: The donor of the graft is from a species different
from the host.
Allograft or homograft: A tissue transfer between individuals of the same
species but with non-identical genes
117.
Autograft: A tissuetransfer from one position to a new position in the same
individual.
Alloplastic graft: A graft of inert synthetic material which is sometimes
called implant material.
118.
Osteoinduction: A processby which the graft material is capable of
promoting cementogenesis, osteogenesis and new periodontal ligament.
Osteoconduction: The graft material acts as a passive matrix, like a trellis or
scaffolding for new bone to cover
119.
MANAGEMENT OF FURCATIONDEFECT
ROOT RESECTION
Root resection may be indicated in multirooted teeth with grade II to IV furcation
involvements.
Root resection may be performed on vital teeth or endodontically treated teeth. It is
preferable, however, to have endodontic therapy completed before resection of a root(s).' ‘
If this is not possible, the pulp should be removed, the patency of the canals determined,
and the pulp chamber medicated before resection.
It is distressing for both patient and clinician to perform a vital root resection and
subsequently have an untoward event occur, such as perforation, fracture of the root, or an
inability to instrument the canal.
120.
The indicationsand contraindications for root resection were well
summarized by Bassaraba.
In general, teeth planned for root resection include the following:
1. Teeth that are of critical importance to the overall dental treatment plan.'
Examples are teeth serving as abutments for fixed or removable restorations for
which loss of the tooth would result in loss of the prosthesis and entail major
prosthetic re-treatment.
2. Teeth that have sufficient attachment remaining for function. Molars with
advanced bone loss in the interproximal and interradicular zones, unless the lesions
have three bony walls, are not candidates for root amputation.
121.
3. Teeth forwhich a more predictable or cost-effective method of therapy is not
available. Examples are teeth with furcation defects that have been treated
successfully with endodontics but now present with a vertical root fracture,
advanced bone loss, or caries on bone root.
4. Teeth in patients with good oral hygiene and low activity for caries are suitable
for root resection. Patients unable or unwilling to perform good oral hygiene and
preventive measures are not suitable candidates for root resection or hemisection.
Root resected teeth require endodontic treatment'-and usually cast restorations
122.
Which Rootto Remove ?
The following is a guide to determining which root should be removed in these
cases:
1. Remove the roots that will eliminate the furcation and allow the production of
a maintainable architecture on the remaining roots.
2. Remove the root with the greatest amount of bone and attachment loss.
Sufficient periodontal attachment must remain after surgery for the tooth to
withstand the functional demands placed on it.
Teeth with uniform advanced horizontal bone loss are not suitable for root
resection
123.
3. Remove theroot that best contributes to the elimination of periodontal problems
on adjacent teeth.
4. Remove the root with the greatest number of anatomic problems, such as severe
curvature, developmental grooves, root flutings, or accessory and multiple root
canals.
5. Remove the root that least complicates future periodontal maintenance
124.
Vital root resectionin severely furcation-involved maxillary molars: Outcomes after up to 7 years
Karin Jepsen, Eva Dommisch, Søren Jepsen, Henrik Dommisch
125.
HEMISECTION
Hemisection isthe splitting of a two-rooted tooth into two separate
portions.
This process has been called bicuspidisation or separation because it
changes the molar into two separate roots.
Hemisection is most likely to be performed on mandibular molars with
buccal and lingual class II or III furcation involvements.
As with root resection, molars with advanced bone loss in the interproximal
and interradicular zones are not good candidates for hemisection.
126.
After sectioningof the teeth, one or both roots can be retained. This decision is
based on the extent and pattern of bony loss, root trunk and root length, ability
to eliminate the osseous defect, and endodontic and restorative considerations.
The anatomy of the mesial roots of mandibular molars often leads to their
extraction and the retention of the distal root to facilitate both endodontic and
restorative therapy.
The interradicular dimension between the two roots of a tooth to be hemisected
is also important. Narrow interradicular zones can complicate the surgical
procedure.
127.
The retentionof both molar roots can complicate the restoration of the
tooth, since it may be virtually impossible to finish margins or to provide
an adequate embrasure between the two roots for effective oral hygiene and
maintenance.
Therefore, orthodontic separation of the roots is often required to allow
restoration with adequate embrasure form.
128.
Hemisection: A conservativemanagement of periodontally involved molar tooth in a young patient Prashant Babaji, Tarun Sihag,1
Vishwajit
Rampratap Chaurasia,2
and Sivaramalingam Senthilnathan3
129.
ROOT RESECTION/HEMISECTION PROCEDURE
The most common root resection involves the distobuccal root of the maxillary first
molar.
After appropriate local anesthesia, a full-thickness mucoperiosteal flap is elevated.
Root resection or hemisection of teeth with advanced attachment loss usually requires
opening both facial and lingual/palatal flaps.
Typically, a root cannot be resected without elevating a flap. the flap should provide
adequate access for visualization and instrumentation and minimize surgical trauma.
After debridement, resection of the root begins with the exposure of the furcation on
the root to be removed. The removal of a small amount of facial or palatal bone may be
required to provide access for elevation and facilitate root removal.
130.
A cutis then directed from just apical to the contact point of the tooth, through
the tooth, and to the facial and distal orifices of the furcation . This cut is made
with a high-speed, surgical-length fissure or crosscut fissure carbide bur.
The placement of a curved periodontal probe into or through the furcation aids in
orienting the angle of the resection.
For hemisection, a vertically oriented cut is made faciolingually through the
buccal and lingual developmental grooves of the tooth, through the pulp chamber,
and through the furcation. If the sectioning cut passes through a metallic
restoration, the metallic portion of the cut should be made before flap elevation.
131.
This preventscontamination of the surgical field with metallic particles. If
a vital root resection is to be performed, a more horizontal cut through the
root is advisable .
An oblique cut exposes a large surface area of the radicular pulp and/or
dental pulp chamber. This can lead to postoperative pain and can
complicate endodontic therapy. A horizontal cut, although it may
complicate root removal, has less postoperative complications.
This root stump can be removed by odontoplasty after the completion of
endodontic therapy or at the time of tooth preparation. After sectioning, the
root is elevated from its socket.
132.
Care shouldbe taken not to traumatize bone on the remaining roots or to
damage an adjacent tooth. Removal of the root provides visibility to the
furcation aspects of the remaining roots and simplifies the debridement of
the furcation with hand, rotary, or ultrasonic instruments.
If necessary, odontoplasty is performed to remove portions of the
developmental ridges and prepare a furcation that is free of any deformity
that would enhance plaque retention or adversely affect plaque removal.
133.
MODERN CLINICAL PROCEDURESIN
PERIODONTAL RECONSTRUCTIVE TREATMENT
Periodontal regeneration is a complex biological process that involves de
novo formation of the lost tooth supporting structures, including alveolar bone,
periodontal ligament, and cementum over a previously diseased root surface
Tissue regeneration depends on the combined presence of progenitor cells,
signaling molecules, blood supply, and scaffolds
Periodontal treatment outcome is usually repair, where healing occurs with a
long epithelial attachment lining most of the previously exposed root surface
and where minimal amounts of new connective tissue attachment, new
cementum and bone are limited only to the apical part of the defect
134.
Reconstructive periodontalprocedures have shown advantage over
conventional surgical procedures in terms of better results in long-term
stability, improved tooth survival, lesser periodontitis progression, and
fewer needs for reintervention over long periods
Clinically, periodontal reconstruction may be achieved by application of
barrier membranes, grafts, wound-healing modifiers, and their
combinations
135.
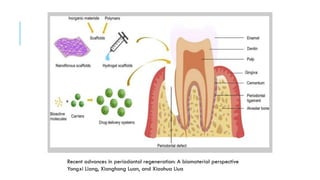
Recent advances inperiodontal regeneration: A biomaterial perspective
Yongxi Liang, Xianghong Luan, and Xiaohua Liua
136.
GUIDED TISSUE REGENERATION
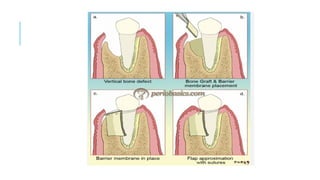
It is a regenerative surgical technique that involves the procedure of raising
mucogingival flap around affected teeth, scaling and planing root surfaces
and placing barrier membranes temporarily under gingiva.
The biological basis of the GTR technique is to block the apical growth of
epithelium to the space over the denuded root surface by using barrier
membrane, therefore facilitating PDL cells and osteoblast to form PDL
tissues and alveolar bone.
138.
Advantages
i. Numerousclinical research have confirmed the benefits of GTR treatments,
including greater clinical attainment level (CAL) gain,
ii. probing pocket depth (PPD) reduction and
iii. bone regeneration compared to open flap debridement (OFD) treatment
Disadvantages
i. Difficulty in treatment of multiple proximal defects,
ii. complications due to membrane exposure
iii.incomplete adaptation of the membrane around irregularly shaped roots
limit their application in reconstructive periodontal surgical procedures
TISSUE ENGINEERING
Dependingon whether biomaterials are used, tissue engineering strategy
for periodontal regeneration can be categorized into scaffold-free and
scaffold-based approaches
For the scaffold-free approach, cells or cell aggregates are transplanted to a
defect area without a cell carrier
141.
Several typesof cells, including bone marrow derived mesenchymal stem
cells (BMSCs) , adipose-derived stem cells (ADSCs), periodontal ligament
stem cells (PDLSCs), and dental pulp stem cells (DPSCs), have been tested
for the potential to form periodontal tissues.
Direct cell implantation faces the problem of cell diffusion out of the defect
area.
Cell sheet technique, which entraps cells in the extracellular matrix (ECM)
secreted by the cells themselves, is capable of preventing cell migration.
142.
BIOMATERIALS
i. ENAMEL MATRIXDERIVATIVE
Enamel matrix protein derivative (EMD) is mainly composed of amelogenins, with smaller
amounts of other non-amelogenin components such as tuftelin, ameloblastin, and enamel proteases
EMD is a biologically active compound that once applied on a denuded root surface starts a
cascade of biologic events, such as enhanced attraction and migration of mesenchymal cells, their
attachment to the root surface, and differentiation into cementoblasts, PDL fibroblasts, and
osteoblasts.
Enamel proteins enhance gene expression responsible for protein and mineralized tissue syntheses
in PDL cells . This process may finally lead to reconstitution of the periodontal apparatus
Histologic evidence of periodontal regeneration, including cementum formation, in humans
following EMD has been extensively reported.
143.
ii. BETA TRICALCIUMPHOSPHATE BONE-REPLACEMENT GRAFT
It has similar chemical composition to the inorganic phase of bone
Bioabsorbable, Osteoconductive
TCP α and TCP β are used
144.
iii.BIPHASIC CALCIUM PHOSPHATE(BCP)
Mixture of HA and TCP in various ratios to adjust degradation rate and
biological activity
Similar chemical composition and structure to the inorganic phase of bone
145.
iv. BIOACTIVE GLASS(BG) Compositions of bioactive glasses vary,
Ions dissolved from BG promote angiogenesis, osteogenesis and antibacterial
activity,
Degradation rate vary over a wide range
146.
v.NATURAL POLYMERS
Collagen- Mostabundant protein in the ECM of alveolar bone, PDL
and cementum, Biocompatible, Low mechanical strength,Safety
problems: pathogen transmission, immune reaction.
Gelatin- Hydrolysis product of collagen, No pathogen transmission
and immune reaction, Easily modified for chemical and light
crosslinking.
Chitosan-Derived from chitin, Biocompatible, Antibacterial property.
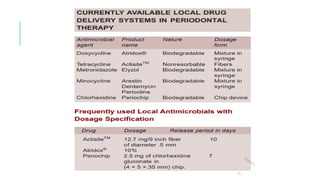
LOCAL DRUG DELIVERYSYSTEMS
The limited efficacy of mouth rinsing and irrigation in deep periodontal pockets led
to the development of alternative delivery systems
The main aim of the drug delivery system is to direct antimicrobials to the infection
sites and maintaining effective level of drugs for sufficient period of time without
eliciting any major side effects.
152.
INDICATIONS
1. As anadjunct in the treatment of few localized nonresponding sites in an
otherwise controlled patient.
2. In ailing and failing implant cases.
3. In medically compromised patients where surgical procedures are not
recommended.
4. Periodontal abscess.
5. Periodontal maintenance therapy.
6. Patient with gastrointestinal intolerance to systemic drug medication
153.
LOCAL ADMINISTRATION OFANTIBIOTICS
AND ANTIMICROBIAL AGENTS
I. Vehicles for local delivery of chemotherapeutic agents include: Dentifrices,
mouth rinses, chewing gum and slow release devices.
154.
METHODS OF DELIVERYOF CHEMOTHERAPEUTIC
AGENTS
a. Keyes technique.
b. Root biomodification.
c. Irrigation devices.
i. Home irrigation devices
• Supragingival home irrigation devices
• Subgingival home irrigation devices
• Marginal home irrigation devices
ii. Professional subgingival irrigation.
155.
KEYES TECHNIQUE
Involves application,by tooth brushing, of a slurry of sodium bicarbonate
and hydrogen peroxide for the control of plaque microorganisms.
Various studies have proved that minimal clinical benefit can be expected
from this technique simply because tooth brushing offers an ineffective
means of delivering medicaments into the periodontal pocket
156.
ROOT BIOMODIFICATION
•Application ofvarious medicaments to root surfaces during surgical therapy
has been evaluated.
•These agents include tetracycline, doxycycline, citric acid and fibronectin.
•Application of these agents on diseased root surfaces during surgery may
enhance connective tissue attachment to the roots, although available data are
inconclusive
157.
Citric acid:
When usedwith pH1 for two to three minutes on root surface, after surgical
debridement, it produces a surface demineralization, which inturn induces
cementogenesis and attachment of collagen fibers.
The following actions of citric acid have been reported by Register and
Burdick in 1975
158.
It removes thesmear layer and may open dentinal tubules, thus allowing
cementum to form within these tubules creating the blunderbuss effect and
produce cementum pins. This could be associated with accelerated
cementogenesis.
It has also been shown to expose collagen fibers on the root surface, which
may splice with the collagen fibers of a soft tissue graft or flap (called as
collagen splicing) resulting in collagen adhesion without cementum
formation and accelerated healing
159.
Epithelium does notmigrate apically because of the accelerated healing
either by connective tissue attachment or a collagen adhesion may occur
before epithelium migrates.
Finally, citric acid, may demineralize small bits of residual calculus,
disinfect the root surface and aid in removing endotoxins
160.
Steps involved:
a. Raisefull thickness flap.
b. Perform thorough root planing.
c. Apply cotton pellets soaked in citric acid pH1 for two to three minutes.
d. Remove and irrigate root surface profusely with water.
e. Replace the flap and suture
161.
HOME IRRIGATION DEVICES
Theadvantage of home irrigation device is, it allows the patient to deliver
medicaments into the periodontal pocket at home on a more frequent basis
than in practice with professional subgingival irrigation
Supragingival home irrigation devices: Results in greater access to
periodontal pockets than mouth rinsing alone. The depth of penetration of
medicament is a maximum penetration of 4 to 5 mm
Subgingival home irrigation devices: Generally includes a blunt ended metal
cannula that the patient inserts into the periodontal pocket
162.
PROFESSIONAL SUBGINGIVAL IRRIGATION
It includes the use of a wide array of powered and manually operated irrigators.
Irrigation using a syringe with a blunt needle has been used.
The most commonly used solutions are chlorhexidine gluconate, stannous fluoride,
tetracycline, metronidazole and hydrogen peroxide
164.
CONCLUSION
A perio-endo lesioncan have a varied pathogenesis which ranges from quite
simple to relatively complex one. Having enough knowledge of these disease
processes is essential in coming to the correct diagnosis
The presence of a combined endodontic-periodontal lesion will always result
in a compromised situation following treatment.
An interdisciplinary approach with a good collaboration between
endodontists, periodontologists and microbiologists, is recommended.
165.
REFERENCES
1. INGLE’S ENDODONTICS6TH
, 7TH
EDITION
2. COHENS PATWAYS OF PULP12TH EDITION
3. ENDODONTIC PERIODONTIC LESION-Igor Tsesis Carlos, E. Nemcovsky, Joseph Nissan, Eyal
Rosen
4. PRINCIPLES AND PRACTICE OF ENDODONTICS 3RD
EDITION- Walter and Torabinejad
5. CARRANZA’S CLINICAL PERIODONTOLOGY- 10th
EDITION- Michael G . Newman, Henry H.
Takei