Cushing's syndrome is caused by excessive cortisol levels due to hyperfunction of the adrenal glands or pituitary gland. It results in central obesity, mood changes, high blood pressure, and other signs and symptoms. The dexamethasone suppression test is used to diagnose Cushing's syndrome by showing that cortisol levels are not suppressed as expected. Addison's disease is caused by primary adrenal insufficiency leading to cortisol and aldosterone deficiencies. Patients present with weakness, low blood pressure, and hyperpigmentation. The short Synacthen test shows no increase in cortisol levels in response to synthetic ACTH stimulation. Both conditions require lifelong hormone replacement therapy and treatment of underlying causes.
Intro to hyperglycemic emergencies - hhs vs dkaPritom Das
Some slides are taken from different textbooks of medicine like Davidson, Kumar and Clark and Oxford, and some from other presentations made by respected tutors. I'm barely responsible for compilation of various resources per my interest. These resources are free for use, and I do not claim any copyright. Hoping knowledge remains free for all, forever.
Intro to hyperglycemic emergencies - hhs vs dkaPritom Das
Some slides are taken from different textbooks of medicine like Davidson, Kumar and Clark and Oxford, and some from other presentations made by respected tutors. I'm barely responsible for compilation of various resources per my interest. These resources are free for use, and I do not claim any copyright. Hoping knowledge remains free for all, forever.
Addison Disease
By Dr Usama Ragab Youssif
The term ‘adrenal insufficiency’ (AI) refers to failure of the adrenal cortex to secrete enough glucocorticoids, mineralocorticoids, or both. AI can be divided into two general categories:
lack of adequate hormone secretion by the adrenals (primary AI)
inadequate ACTH or CRH secretion (secondary AI).
1. Adrenal Revision
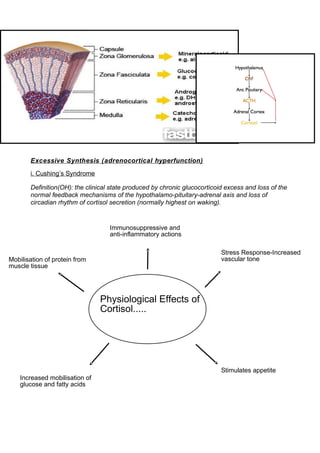
Excessive Synthesis (adrenocortical hyperfunction)
i. Cushing’s Syndrome
Definition(OH): the clinical state produced by chronic glucocorticoid excess and loss of the
normal feedback mechanisms of the hypothalamo-pituitary-adrenal axis and loss of
circadian rhythm of cortisol secretion (normally highest on waking).
Physiological Effects of
Cortisol.....
Stress Response-Increased
vascular tone
Stimulates appetite
Increased mobilisation of
glucose and fatty acids
Immunosuppressive and
anti-inflammatory actions
Mobilisation of protein from
muscle tissue
2. Think about the physiological effects of cortisol and what symptoms/signs this might
produce:
Signs
Central obesity
Plethoric (red) moon face
Buffalo neck hump
Supraclavicular fat pads
Skin and muscle atrophy
Bruises
Purple abdominal striae
Osteoporosis
Hypertension
Hyperglycaemia
Infection prone-poor healing.
Symptoms
Increase in weight
Mood change (depression, lethargy, irritability)
Weakness
Irregular periods
Facial hair growth (in females)
Erectile dysfunction
recurrent Achilles tendon rupture
3. What are the causes?
• Iatrogenic
The commonest cause is oral steroid treatment (i.e. after long-term treatment with
prednisolone and dexamethasone)
• Endogenous
The endogenous causes can be divided into:
-Adrenal origin (excess cortisol production by an adrenal cortical neoplasm, e.g. adrenal
nodular hyperplasia)
-Pituitary origin (excess ACTH production by a pituitary neoplasm-Cushing’s disease)
-Ectopic origin (excess ACTH production by a non-pituitary neoplasm, especially small cell
lung cancer and carcinoid tumours).
How do you tell which is which?
• dexamethasone suppression test: in Cushing’s syndrome the cortisol does not fall as we
would expect it to.
• to work out where the lesion is-do a plasma ACTH; if it is undetectable, then the excess
cortisol must be coming from the Adrenals (as the pituitary is still responding to negative
feedback, resulting in the low/undetectable levels of ACTH, but the adrenals are out of
control)
• if ACTH is detectable, to distinguish between a pituitary and an ectopic cause, we need
to do a high-dose dexamethasone suppression test; complete or partial suppression of
the cortisol levels indicates a pituitary cause as the pituitary retains some feedback
control.
Treatment?
• Iatrogenic: Stop oral steroids if possible
4. • Endogenous: Selective removal of the offending neoplasm if possible; bilateral
adrenalectomy if source unlocatable, recurrence post-op, or adrenal adenoma/carcinoma
present.
ii. Conn’s Syndrome
• Primary hyperaldosteronism (Conn Syndrome) is usually caused by an aldosterone-
secreting adrenal adenoma.
*Key thing to remember regarding Conn Syndrome: it causes hypertension,
neuromuscular symptoms and renal potassium wasting due to elevated levels of
aldosterone (if you think about what aldosterone does, it makes sense).
iii. Adrenogenital Syndromes
• Congenital adrenal hyperplasia-95% of cases are due to partial or complete deficiency in
21-hydroxylase.
• The deficiency in this enzyme involved in the biosynthesis of adrenal steroids (i.e.
cortisol) means that steroidogenesis is then channelled into other pathways, leading to
excess production of androgens.
*The 3 most common syndromes are characterised by virilism-the newborn female infant
may present with pseudohermaphrodism, while precocious puberty occurs in affected
males.
*Some defects also affect aldosterone synthesis (i.e. low aldosterone as well as low
cortisol), causing salt wasting which can be life-threatening in the newborn.
Adrenal insufficiency
i.Addison’s Disease
Definition (OH): primary adrenocortical insufficiency; destruction of the adrenal cortex
leads to glucocorticoid (cortisol) and mineralocorticoid (aldosterone) deficiency.
What are the causes?
Surgical Sieve is helpful here:
5. • V vascular-perinatal haemorrhagic necrosis, adrenal haemorrhage (Waterhouse-
Friderichsen syndrome), post partum adrenal infarction
• I infection/inflammatory-chronic infections (T.B. is commonest cause worldwide),
sarcoidosis
• T trauma-traumatic necrosis
• A auto-immune-auto-immune adrenalitis (60-70%, now commonest cause in U.K.)
• M metabolic-amyloidosis (not really a metabolic condition but may help to remember it
here, or you can just remember it on it’s own)
• I iatrogenic-abrupt withdrawal of corticosteroid treatment
• N neoplastic-disseminated metastatic carcinoma (lung, breast)
Presentation
• If it helps you can remember this slide and the 5 T’s:
Or this list:
• weakness
• nausea & vomiting
• abdominal pain
• weight loss
• hyperpigmentation of the skin (check palmar creases) & mucous membranes
• hypotension-dizziness and faints.
• Vitiligo
Remember these electrolyte disturbances:
Hb 12.5 g/dL normal
6. Na+ 125 mmol/L (low)
K+ 6.5mmol/L (high)
Ur 10mmol/L (high)
Glucose 2.9 mmol/L (low)
Investigations:
• Short Synacthen Test-an injection of synacthen should cause a normal rise of cortisol in
30 minutes (cortisol measurement after 30 minutes should be >550nmol/L)
Treatment:
• Corticosteroid Replacement (hydrocortisone daily)
• Mineralocorticoid replacement may be needed as well (fludrocortisone daily)
• Warn against abruptly stopping steroids, and advise about need to increase doses in
illness/stress
• Give steroid card
Management of an Addisonian Crisis:
D-assess for danger
R-assess for a response (pt may be very weak and confused)
A-Airways-look, listen, feel.
B-Breathing-look, listen, feel, measure (O2 sats), treat (oxygen)
C-Circulation-look (pallor, oedema, bleeding), listen (heart sounds-may be soft), measure
(BP-they are likely to be hypotensive, HR-feeble rapid pulse, UO-may be oliguric, Temp-
7. pyrexia is common and may be due to underlying infection, Cap refill), treat (obtain iv
access, give bolus of normal saline, take bloods)
D-Disability-AVPU score, measure serum glucose
E-Exposure-hyperpigmentation/medic alert bracelet may give you some clues!
• If an Addisonian crisis is suspected, treat without waiting for biochemical results
• Take blood for cortisol and ACTH if possible
• Give Hydrocortisone sodium succinate 100mg stat.
• Glucose iv may be needed if hypoglycaemic
• Continue iv fluids to correct dehydration, as guided by clinical state. Correct electrolyte
imbalances.
• Continue hydrocortisone sodium succinate e.g. 100mg/6h iv.
• Change to oral steroids after 72 hrs if patient’s condition is good.
• Fludrocortisone may be needed as well.
• Search for and treat the underlying cause (Infection, trauma. abrupt withdrawal of
steroids)
Key Points
• In Cushing’s syndrome you have an excess of Cortisol
• To investigate this you do the dexamethasone suppression test (because you are
trying to see if the excess levels can be suppressed)
• In Addison’s disease you have Adrenal insufficiency
• This results in characteristic features including hyperpigmentation, nausea & vomiting,
weakness and hypotension.
• You get low sodium and low glucose
• You get high potassium and raised urea
• To investigate this you do the short synacthen test (because you are trying to see if
synthetic ACTH will stimulate cortisol release)