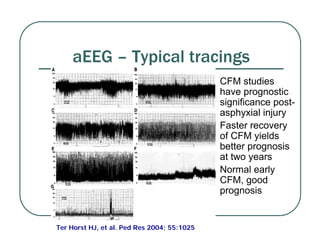
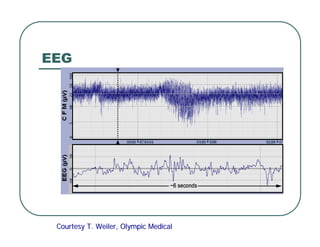
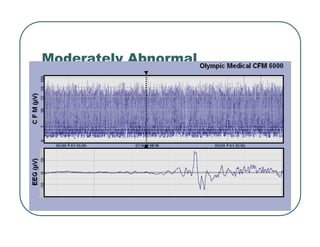
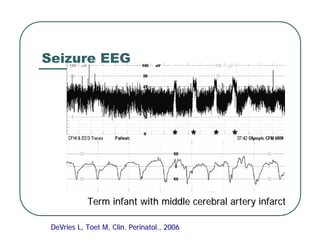
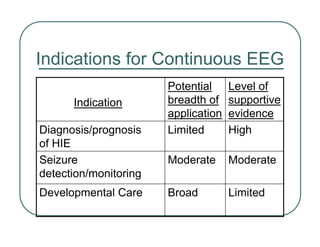
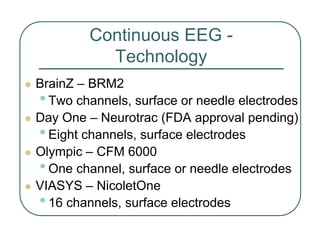
The document discusses continuous EEG monitoring in newborns, highlighting its importance in diagnosing, prognosing, and monitoring seizures, particularly following hypoxic-ischemic events. It outlines the capabilities of different EEG technologies, the types of EEG activities observed, and the potential risks and benefits in clinical settings. The text emphasizes the need for professional training and the cautious application of EEG monitoring to improve neonatal care while avoiding unnecessary interventions.