Download as PPSX, PPTX







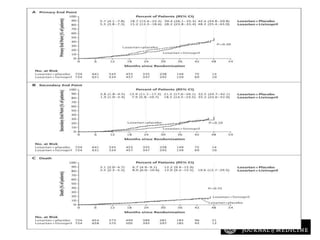
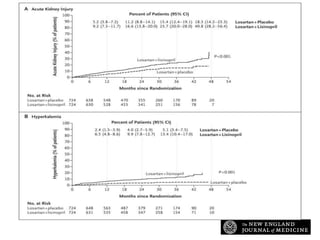

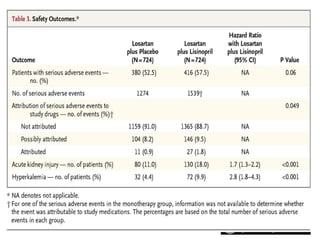


The VA NEPHRON-D study investigated the efficacy and safety of combination therapy with losartan and lisinopril compared to losartan alone for treating diabetic nephropathy. The study was stopped early due to a higher risk of hyperkalemia and acute kidney injury with combination therapy. While combination therapy further reduced proteinuria, it did not provide significant renal protection and led to more adverse events compared to losartan alone. Therefore, combination renin-angiotensin system blockade is not recommended for treating diabetic nephropathy.















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














