Downloaded 31 times

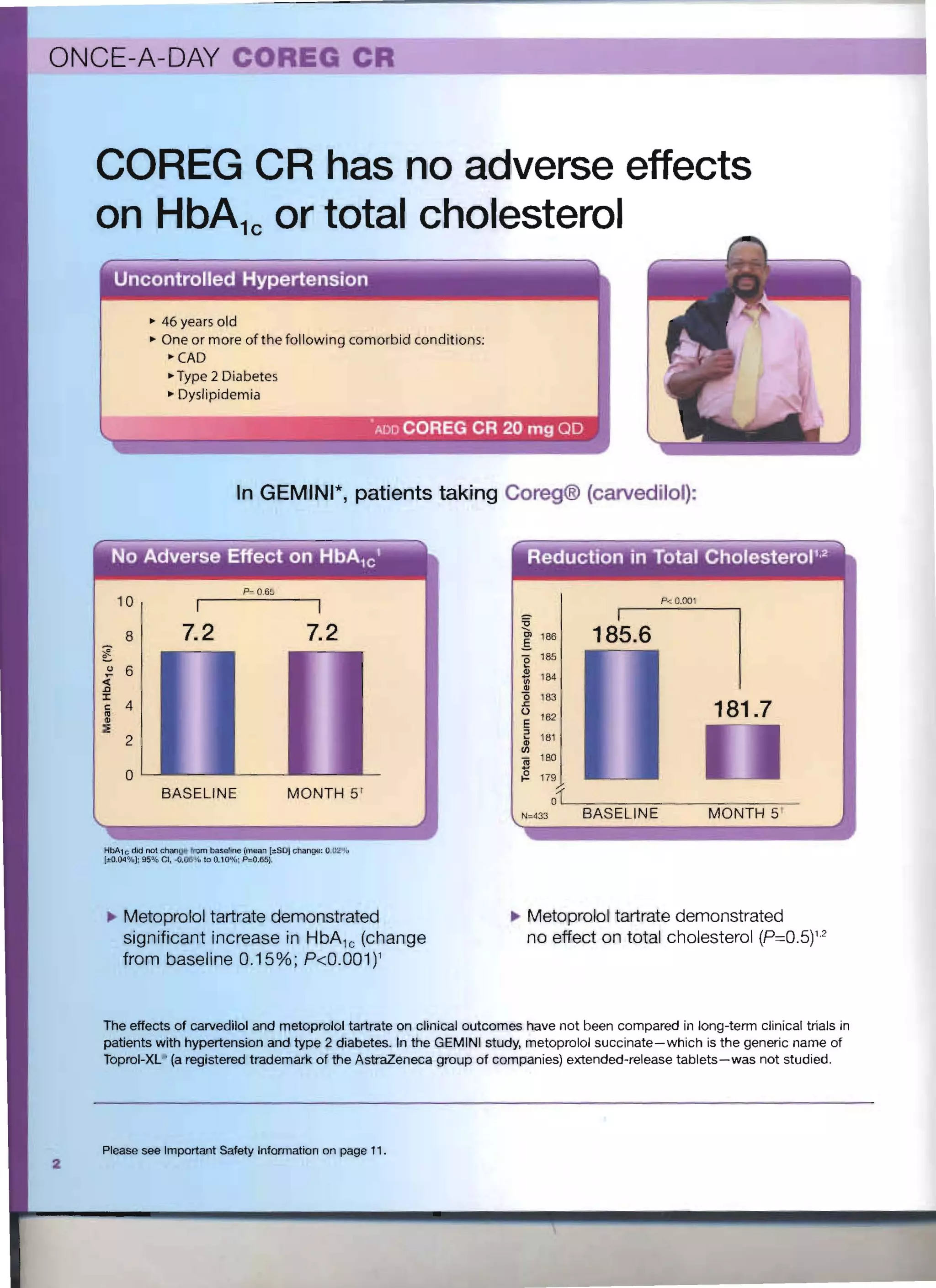






1) COREG CR is an extended-release capsule formulation of carvedilol for once-daily dosing in patients with type 2 diabetes and hypertension. 2) In clinical trials, COREG CR lowered blood pressure without affecting metabolic parameters like HbA1c and cholesterol levels. 3) COREG CR did not have adverse effects on triglycerides or weight compared to other hypertension drugs.













































































