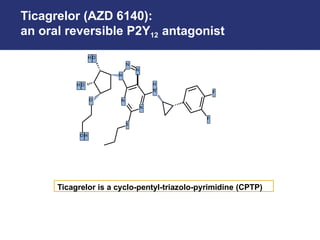
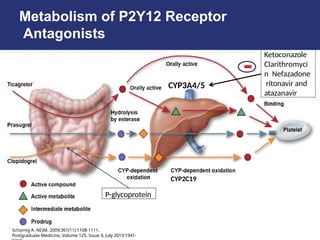
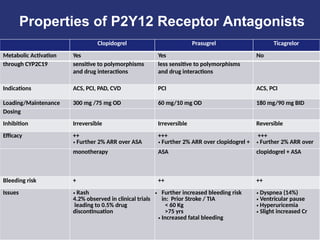
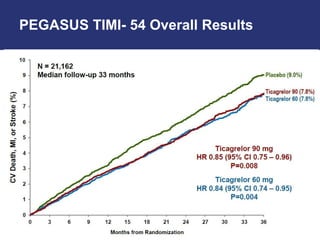
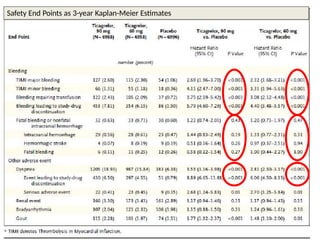
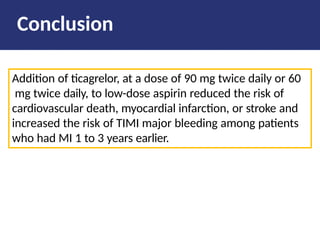
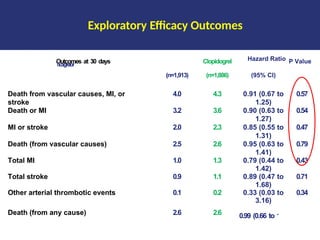
Ticagrelor is a reversible P2Y12 antagonist that offers advantages over clopidogrel, including faster onset and greater platelet inhibition, leading to reduced ischemic events in acute coronary syndrome patients. Studies show that while ticagrelor reduces myocardial infarction and stent thrombosis, it may also increase bleeding risk, particularly in certain populations. The evidence supports ticagrelor as a superior alternative to clopidogrel, especially for patients undergoing percutaneous coronary intervention.




































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)