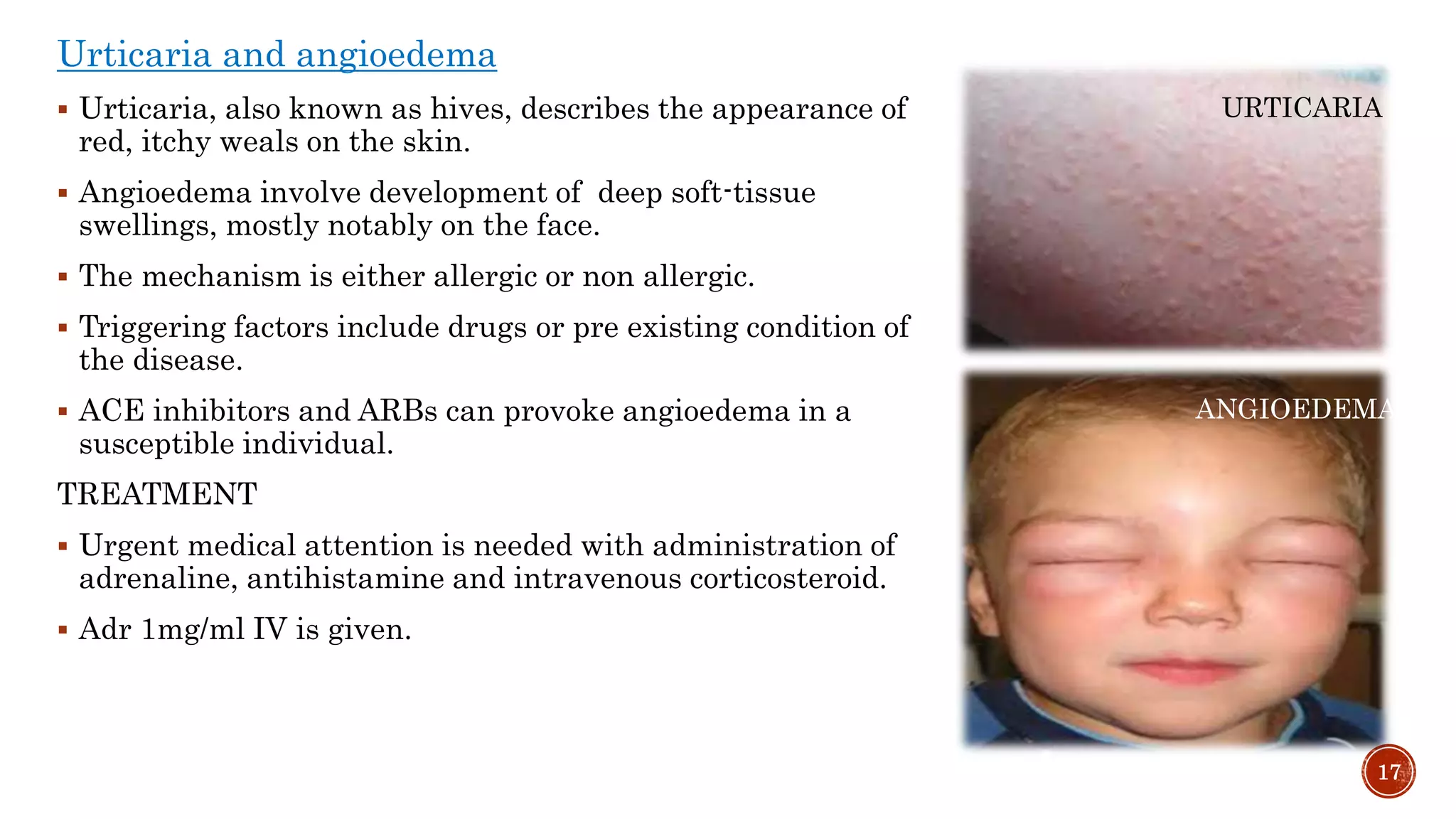
Drug-induced skin reactions are common, accounting for 30% of all reported adverse drug reactions. The document discusses the epidemiology, etiology, pathophysiology, diagnosis, clinical presentations, and treatment of various drug-induced skin disorders. Mild disorders include exanthems, urticaria, fixed drug eruptions, and pruritus, while more severe disorders include erythema multiforme and erythema nodosum. Common culprit drugs are antibiotics, anticonvulsants, and NSAIDs. Treatment involves identifying and withdrawing the offending agent when possible along with symptomatic relief.






























































![Cutaneous Drug Reactions [Autosaved].ppt 2.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/cutaneousdrugreactionsautosaved-251014081902-3f3a2e35-thumbnail.jpg?width=640&height=640&fit=bounds)





























