2. CONTENTS
• ANATOMY OF THE ANAL REGION
• INTRODUCTION
• CLASSIFICATION
• CLINICAL ASSESSMENT
• IMAGING STUDIES
• MANAGEMENT
• TAKE HOME MESSAGE
• REFERENCES
3. ANATOMY
• The anal canal, as defined by the
surgeon/clinician, is approximately 4 cm in
length, extending from the anal verge to the
top of anorectal ring.
• Anatomist considers the anus to be the 2 cm
from the anal verge to the dentate line.
Bailey and love textbook of surgery, 27th edition
4. INTERNAL ANAL SPHINCTER EXTERNAL ANAL SPHINCTER
Thickened (2–5 mm) distal continuation of the
circular muscle coat of the rectum.
The external anal sphincter is a funnel shaped
structure composed of the pelvic floor muscles
enveloping the distal rectum and anus
This is involuntary muscle. Voluntary muscle
The internal anal sphincter is supplied by
sympathetic (L5) and parasympathetic (S2, S3,
and S4) nerves
The external anal sphincter is innervated on
each side by the inferior rectal branch of the
pudendal nerve (S2 and S3) and by the
perineal branch of S4.
SUBDIVIDED INTO:
• Deep
• Superficial
• subcutaneous
6. FISTULA-IN-ANO
DEFINITION:
It is a chronic abnormal communication, usually lined to some degree by
granulation tissue, which runs outwards from the anorectal lumen (the internal
opening) to an external opening on the skin of the perineum or buttock (or rarely, in
women, to the vagina).
• Drainage of an anorectal abscess results in cure for about 50% of patients. The
remaining 50% develop a persistent fistula in ano.
7. Epidemiology
• The overall incidence is about 9 cases per 100 000 population per year in western
Europe.
• Age: third, fourth and fifth decades of life are most commonly affected
• Sex: More common in men than women.
8. ETIOLOGY
The most common etiology of an anorectal fistula is an infected anal crypt gland.
May be found in association with specific conditions, such as
• Crohn’s disease,
• Tuberculosis,
• Lymphogranuloma venereum,
• Actinomycosis,
• Rectal duplication,
• Foreign body and
• Malignancy
• Non-specific, idiopathic or cryptoglandular, and intersphincteric anal gland infection
is deemed central to them.
10. Park’s classification
Based on the centrality of intersphincteric
anal gland sepsis (the internal opening is
usually at the dentate line), which results
in a primary track whose relation to the
external sphincter defines the type of
fistula and which influences management
Sabiston’s textbook of surgery-21st Edition
11. INTERSPHINCTERIC: TRANSSPHINCTERIC
• 45% 30%
• Do not cross the external sphincter Have a primary track that crosses both internal and
external sphincters (the latter at a variable level) and
which then passes through the ischiorectal fossa to
reach the skin of the buttock.
• Most commonly they run directly from the internal
to the external openings across the distal internal
sphincter
• But may extend proximally in the intersphincteric
plane to end blindly with or without an abscess
(high blind tract), or
• Rectal opening without perineal opening
12. SUPRASPHINCTERIC FISTULAE EXTRASPHINCTERIC FISTULAE
Very rare • Run without specific relation to the
sphincters
• Fistula originates at the anal crypt and
encircles the entire sphincter apparatus,
and terminates in the ischiorectal fossa
Iatrogenic • Typically not cryptoglandular in origin
• Result from pelvic disease or trauma
Difficult to distinguish from
high-level trans-sphincteric tracks
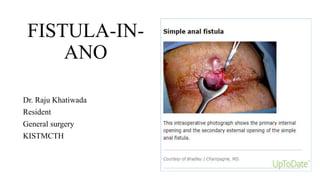
13. Simple fistulas
• Low-lying transsphincteric (Parks' type 2 and involving <30 percent of anal
sphincter complex) and
• Intersphincteric fistulas (Parks' type 1)
• Traditional approach to treatment is primary fistulotomy
14. Complex fistula
A complex fistula refers to those fistulas that have a
• high risk of treatment failure and
• cannot be safely treated by routine fistulotomy.
15. An anal fistula is defined as complex in the
following situations:
• Any fistula involving more than 30 percent of the external sphincter
• Suprasphincteric fistulas
• Extrasphincteric or high fistulas, proximal to the dentate or pectinate line
• Women with anterior fistulas
• Fistulas with multiple tracts
• Recurrent fistulas
• Fistulas related to inflammatory bowel disease
• Fistulas related to infectious diseases, including tuberculosis and HIV
• Fistulas secondary to local radiation treatments
• Patients with a history of anal incontinence
• Rectovaginal fistulas
16. CLINICAL PRESENTATION
• Patients usually complain of intermittent purulent discharge (which may be
bloody)
• Rectal pain (which increases until temporary relief occurs when the pus
discharges).
• There is often, but not invariably, a previous episode of acute anorectal sepsis that
settled (incompletely) spontaneously or with antibiotics, or which was surgically
drained.
• The passage of flatus or faeces through the external opening is suggestive of a
rectal rather than an anal internal opening.
17. PHYSICAL EXAMINATION:
• Perianal skin may be excoriated and inflamed
• An indurated tract is often palpable
• Palpable cord leading from the external opening to the anal canal may be present
18. The key points in physical examination
• To determine the site of the internal opening;
• The site of the external opening(s)
• The course of the primary track
• The presence of secondary extensions; and
• The presence of other conditions complicating the fistula.
• Palpable induration between external opening and anal margin suggests a
relatively superficial track,
• Whereas supralevator induration suggests a primary track above the levators or
high in the roof of the ischiorectal fossa, or a high secondary extension.
• Intersphincteric fistulae usually have an external opening close to the anal verge.
19. Goodsall’s rule
• Although the external opening is often
easily identifiable, identification of the
internal opening may be more
challenging
• Goodsall’s rule can be used as a guide
in determining the location of the
internal opening
20. • Full examination under anaesthesia (EUA)
should be repeated before surgical
intervention.
• Dilute hydrogen peroxide, instilled via the
external opening
• Gentle use of probes and a finger in the
anorectum usually delineates primary and
secondary tracks and their relations to the
sphincters.
21. IMAGING STUDIES
• Pelvic MRI is ‘gold standard’ for fistula imaging
• The great advantage of MRI is, it demonstrates
secondary extensions, which may be missed at
surgery and which are the cause of persistence
and delineate the anatomy of the fistula tracks
• Anal fistulography and computed tomography
(CT) both have limitations but are useful
techniques if an extrasphincteric fistula is
suspected.
• Endoanal ultrasound, gives information about
sphincter integrity
22. A meta-analysis showed that, for assessment of anal fistulas, MRI has a sensitivity
of 87 percent and a specificity of 69 percent;
EUS has a sensitivity of 87 percent and a specificity of 43 percent
Siddiqui MR, Ashrafian H, et al. A diagnostic accuracy meta-analysis of endoanal ultrasound and MRI for
perianal fistula assessment. Dis Colon Rectum. 2012 May;55(5):576-85. doi: 10.1097/DCR.0b013e318249d26c.
PMID: 22513437.
23. Management
Surgery is the mainstay of therapy with the ultimate goal of
Draining local infection,
Eradicating the fistulous tract, and
Avoiding recurrence while preserving native sphincter function.
• The surgical approach depends upon correct classification of the fistula
• Alternatively, a draining seton may be used to keep the fistula tract open, which
often prevents recurrent abscess
24. SURGICAL MANAGEMENT
Simple intersphincteric fistulas:
can often be treated by lay-open fistulotomy (opening the fistulous tract), curettage,
and healing by secondary intention
Complex fistula:
• Draining seton placed to preserve the sphincter mechanism and help eradicate the
septic focus.
• In six or more weeks, a second sphincter-sparing procedure can be performed after
drainage diminishes
25. Procedure selection
High transsphincteric fistula:
either an Endoanal advancement flap or LIFT
Suprasphincteric fistula:
Suprasphincteric fistulas (Parks' type 3) should be treated with Endoanal
advancement flaps. LIFT is not an option, because there is no intersphincteric fistula
tract.
Extrasphincteric fistula:
Extrasphincteric fistulas (Parks' type 4) are typically not of cryptoglandular origin
but are instead caused by cancer or Crohn disease. These fistulas are rare but
difficult to treat. Surgical options include proctectomy or fecal diversion.
26. Recurrent fistula:
• Recurrent fistulas that involve the sphincter complex typically warrant a pelvic
magnetic resonance imaging (MRI) scan to clarify anatomy and a seton for
drainage.
• Managed according to their classification
28. FISTULOTOMY
• It involves division of all those structures lying between the external and internal
openings.
• It is therefore applied mainly to intersphincteric fistulae and trans-sphincteric
fistulae involving less than 30% of the voluntary musculature (simple fistulae)
• If the fistula tract courses higher into the sphincter mechanism, seton placement is
done
• Patients should be observed for a minimum of six months following the procedure
before determining a treatment failure or success
29. Fistulotomy
• The recurrence rate for treatment of
simple anal fistulas with fistulotomy is
2% to 8% and
• Functional impairment generally
between 0% and 17%.
30. Fistulectomy
• Excision of the fistula
• Complete fistulectomy creates larger wound that takes lomger to heal and offers
no recurrence advantage over fistulotomy
• Diathermy cautery is used
• It allows better definition of fistula anatomy than fistulotomy, especially the level
at which the track crosses the sphincters and the presence of secondary extensions.
31. Seton
• Seton is a thread of nylon, prolene, rubber
or other material that is non-absorbable and
is placed through the fistula track with the
purpose of keeping it open for certain
period of time
• Can be Loose seton or tight/cutting seton
32. USES OF LOOSE SETONS
• For long-term palliation: to avoid septic and painful exacerbations by
establishing effective drainage; most often in Crohn’s disease
• Used before ‘advanced’ techniques (fistulectomy, advancement flap, cutting
seton): acute sepsis and secondary extensions are eradicated and a loose seton is
passed across the sphincteric component of the primary track to simplify the
fistula and allow fibrosis.
• As part of a staged fistulotomy.
• As part of a therapeutic strategy to preserve the external sphincter in trans-
sphincteric fistulae.
33. Cutting setons
• Cutting setons placed through the fistula and intermittently tightened in the office.
• Tightening the seton results in fibrosis and gradual division of the sphincter, thus
eliminating the fistula while maintaining continuity of the sphincter
• The two most important complications of a fistulotomy with a snug seton (cutting)
are recurrence and incontinence.
• The success rates for snug setons range from 82 to 100 percent; however, long-
term incontinence rates can exceed 30 percent
Patton V, Chen CM, Lubowski D. Long-term results of the cutting seton for high anal fistula. ANZ J Surg. 2015
Oct;85(10):720-7. doi: 10.1111/ans.13156. Epub 2015 May 21. PMID: 25997475.
34. Endorectal advancement flap
• Higher fistulas may be treated by an endorectal advancement flap
• The endoanal and endorectal advancement flaps preserve the anal sphincter by
closing off the internal opening of the fistula by a mobilized flap of healthy tissue
• The key component of this procedure is to create a flap that includes the mucosa,
submucosa, and a portion of the circular muscular fibers that is sufficient to cover
the internal opening.
• The base of the flap proximally should measure at least twice its width at the apex.
35. Outcome of Endorectal advancement flap
A variety of endoanal advancement flap techniques exist and, in experienced hands,
have low-to-moderate recurrence rates (0 to 40 percent), depending in part on
patient population, and tolerable incontinence rates ranging from 0 to 12.5 percent
van Koperen PJ, Wind J, Bemelman WA, Bakx R, Reitsma JB, Slors JF. Long-term functional
outcome and risk factors for recurrence after surgical treatment for low and high perianal fistulas
of cryptoglandular origin. Dis Colon Rectum. 2008 Oct;51(10):1475-81. doi: 10.1007/s10350-008-
9354-9. Epub 2008 Jul 15. PMID: 18626715.
36. LIFT (ligation of the intersphincteric fistula
tract)
• Sphincter-preserving procedure, first described in 2006 for trans-sphincteric
fistulae.
• The technique involves disconnection of the internal opening from the fistula tract
at the level of the intersphincteric plane and removal of the residual infected
glands without diving any part of the sphincter complex.
• The tract is then ligated and divided, the internal part is removed and the external
part of the track is curretted out and drained.
• Success in terms of healing have been quoted at anything from 47% to 95%.
37. LIFT
• LIFT can be used to treat both simple and
complex fistulas.
• Fistula tract longer than 3 cm, previous
procedures, and obesity have been
associated with LIFT failure
• Outcomes data vary depending on the type
of fistulas.
• Meta-analyses report that the standard
LIFT procedure achieved fistula healing in
61 to 94 percent of patients in four to eight
weeks, with low morbidity (14 percent)
and rare fecal incontinence (1.4 percent)
Hong KD, Kang S, Kalaskar S, Wexner SD. Ligation of intersphincteric fistula tract (LIFT) to treat anal fistula:
systematic review and meta-analysis. Tech Coloproctol. 2014 Aug;18(8):685-91. doi: 10.1007/s10151-014-1183-3.
Epub 2014 Jun 24. PMID: 24957361.
39. Take home message
• Confirmation of the anatomy of the fistula
• Surgical management is the mainstay of therapy
• Use staged procedure
• Reduce to a simple tract- using draining seton
• Use non diversion technique
• Patients with a recurrent fistula require a pelvic magnetic resonance imaging
(MRI) scan to clarify anatomy and a seton for drainage
• Reassess the situation after each intervention
40. REFERENCES
• Bailey and love textbook of surgery, 27th edition
• Sabiston’s textbook of surgery-21st Edition
• Schwartz textbook of surgery, 11th edition.
• Uptodate