
Uploaded byNaghmeh Foroutan
DPP-4-inhibitors-CAPT 2015- Toronto- poster presentation
This systematic review and meta-analysis compared the safety and efficacy of dipeptidyl peptidase-4 (DPP-4) inhibitors versus sulfonylureas as second-line adjunctive therapy for type 2 diabetes patients inadequately controlled with metformin. The analysis found no significant difference in efficacy (HbA1c change) between the two classes, but patients on DPP-4 inhibitors experienced significantly fewer hypoglycemic events. Future research should focus on the economic implications of DPP-4 inhibitors compared to sulfonylureas in this patient population.
More Related Content







![Iv To Po Pp[1]](https://cdn.slidesharecdn.com/ss_thumbnails/ivtopopp1-090518013206-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

















Similar to DPP-4-inhibitors-CAPT 2015- Toronto- poster presentation






























DPP-4-inhibitors-CAPT 2015- Toronto- poster presentation
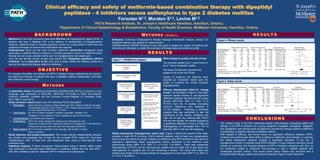
- 1. Clinical efficacy andsafety of metformin-based combination therapy with dipeptidyl peptidase - 4 inhibitors versus sulfonylurea in type 2 diabetes mellitus Foroutan N1,2, Muratov S1,2, Levine M1,2 1PATH Research Institute, St. Joseph’s Healthcare Hamilton, Hamilton, Ontario; 2Department of Clinical Epidemiology & Biostatistics, Faculty of Health Sciences, McMaster University, Hamilton, Ontario R E S U LT S BAC KG RO U N D To compare the safety and efficacy of DPP-4 inhibitors versus sulfonylurea as second- line adjunctive therapy in patients with type 2 diabetes mellitus inadequately controlled with metformin mono-therapy. • Metformin is the most commonly prescribed first-line oral hyperglycemic agent (OHA) in patients with type 2 diabetes with a low potency of development of hypoglycaemia. However, metformin fails to maintain glycemic control for a long period of time and thus additional therapies as second-line medications are required. • Sulfonylureas (SUs) are the most common adjunctive second-line therapeutic drugs particularly in patients failing to achieve or maintain glycaemic control on metformin mono- therapy but can cause adverse events such as hypoglycaemia and weight gain. • Over the last decade clinical studies have shown that “Dipeptidyl peptidases (DPP)-4 inhibitors” as an alternative to SU may have a better safety and efficacy profile as a second-line adjunctive therapy added to metformin. O B J E C T I V E Methodological quality and risk of bias The included studies (Fig 1.) were found to be of “low to moderate” quality. The body of evidence in general was judged to be at low risk of bias Quality of evidence per outcome were reported as “moderate” based upon the quality of evidence for critical outcome (hypoglycemia) C O N C LU S I O N S M E T H O D S • A systematic review of published randomised controlled trials (RCTs) in humans, in any language, was performed in MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, EMBASE, PubMed and the Cochrane Central Register of Controlled Trials from 1980 to June 2015. • Study inclusion criteria based upon the following PICOS description: Population: adults with type 2 diabetes mellitus requiring an OHA added to metformin because of inadequate glycemic control (HbA1c > 6.5%, fasting plasma glucose >7 mmol/L or 2-hour postprandial glucose > 10 mmol/L) Intervention: any DPP-4 inhibitor (alogliptin, linagliptin, saxagliptin, sitagliptin, and vildagliptin), in the treatment of type 2 diabetes (as second-line therapy) Comparator(s): any Sulfonylurea compound Outcome(s): HbA1c (%) (mean change from baseline) and Hypoglycemic event (proportion of patients who experienced at least one hypoglycemic event defined as a finger-stick glucose value ≤50 mg/dl with associated symptoms) Study type(s): RCTs in humans, published in any language, with at least 12 weeks follow-up duration. • Study selection and quality assessment: Two review authors independently selected the studies and assessed risk of bias for the included RCTs using the “Cochrane Collaboration’s Risk of Bias tool” and abstracted data using a study-specific data extraction form. • Statistical analysis: A direct comparison meta-analysis using a random effect model was conducted to calculate mean differences in treatment effects and risk ratio (RR) - with 95% confidence interval- between DPP-4 inhibitors and sulfonylurea. Figure 2: Efficacy results Figure 3: Safety results Records identified through database searching (n =3561) Records after duplicates removed (n = 3081) Records excluded not meeting inclusion criteria (n =3047) Full-text articles assessed for eligibility (n = 34) Full-text articles excluded, with reasons (n =24) - Non-RCTs (n=9) - Conference proceedings & unpublished trials (n=3) - Trials do not meet inclusion (PICOS) criteria (n=6) - Same study with multiple articles (n=3) - Post-hoc analyses (n=2) - <12 week follow-up (n=1) Studies included in qualitative synthesis (n =10) Studies included in quantitative synthesis (meta-analysis) (n = 10) Records passed title & abstract screening (n = 34) Figure 1 : PRISMA flow diagram Efficacy Assessment (HbA1c% change score) : As illustrated in figure 2, the meta- analysis results showed a non-significant difference between the test and the control groups (MD=0.06, 95% CI -0.00- 0.13, P=0.07) from the 10 studies evaluating HbA1c% (difference from baseline) in 10,139 subjects. Following a sensitivity analysis that was performed to test the robustness of the results, stratifying into high risk of bias (for missing data >20%) and low risk studies, the results changed to a significant difference in favor of SUs and heterogeneity (I2) decreased from 73% to less than 48% in the low risk subgroup. Safety assessment (hypoglycemic event rate): Figure 3 shows the results of the meta- analysis of eight RCTs involving 10,616 diabetic patients, with at least one hypoglycemic event during the follow-up period. Patients on metformin plus DPP-4inhibitors were found to experience significantly fewer hypoglycemic events compared to the metformin plus sulfonylurea group (RR= 0.15; 95% CI, 0.11-0.22; P<0.00001). There was substantial heterogeneity (I2=77%), but by removing two outliers and one high risk of bias study, the heterogeneity (I2) equaled zero for the remaining 5 studies. The result from these five studies was similar to the 8 study analysis for hypoglycemic event rates (RR= 0.12; 95% CI, 0.1-0.15; P<0.00001). • The present study is the first systematic-review/ meta-analysis comparing safety and efficacy of all DPP-4 inhibitors as a group (alogliptin, linagliptin, saxagliptin, sitagliptin, and vildagliptin) with sulfonylureas as adjunctive second-line therapy added to metformin monotherapy in patients with type 2 diabetes mellitus. • With respect to efficacy, the review shows no significant difference between DPP4- inhibitors and sulfonylurea when either is added to metformin mono-therapy. In contrast, the safety assessment analysis showed a significant decrease in the risk of hypoglycemic events in patients using DPP4-inhibitors. Future research activities should include an economic and financial analysis of DPP-4 inhibitors compared with SUs, as the medication added to metformin mono-therapy in type 2 diabetic patients with inadequate glycemic control. That would inform policy makers and clinicians with a comprehensive efficacy, safety and economic-financial impact of each treatment. Softwares: Cochrane Collaboration’s Review Manager (RevMan®) Analysis Version 5.3 statistical software was applied for meta-analysis. GRADEprofiler® (GRADE Working Group) was used to assess the quality of evidence per outcome and ultimately to create the summary of findings table and evidence profile. M E T H O D S ( C O N T. )