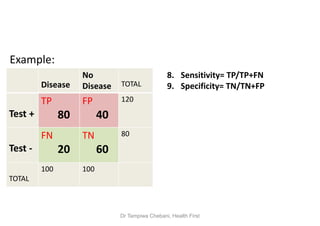
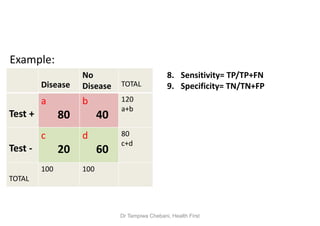
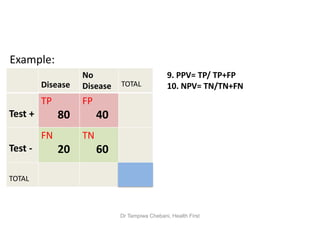
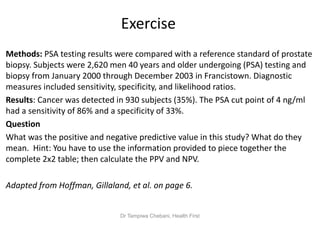
The document discusses the importance and validity of screening tests in healthcare, highlighting their role in identifying asymptomatic diseases within populations. It outlines criteria for effective screening tests, including sensitivity, specificity, and predictive values, and addresses potential disadvantages such as over-diagnosis and false positives/negatives. Additionally, it explains how the prevalence of a condition affects the predictive values of test results.