Downloaded 82 times

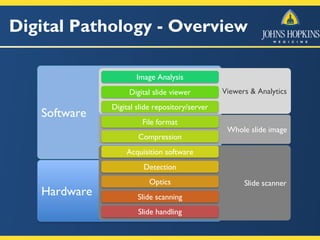





The document discusses the applications and considerations of digital pathology at Johns Hopkins, highlighting whole slide imaging, live imaging, and various clinical uses including education, research, and primary diagnosis. It outlines scanner considerations, digital slide file formats, and the differences between research and clinical implementations. The focus is on developing infrastructure for analytics and efficient practices in pathology, emphasizing collaborative and educational resources.



































































