Differential leukocytic count 2 in clinical practice
2.
Case
:
• 32 yearsold male patient , driver , returned from al Kuwait 3 months ago
for vacation , referred from urology clinic to hematology clinic due to
persistent leukocytosis in routine CBC check up before stone extraction
procedure , the patient was given repeated courses of antibiotics without
any improvement of the leukocytosis .
3.
• By examination: the patient is generally well and fit, BP 120/80 mmHg ,
pulse 95 , with no pallor , cyanosis or change in complexion .
• Cardiac auscultation revealed pansystolic murmur over the apex propagated
to axilla and with ejection systolic murmur over the pulmonary area .
• lung field examination was free .
• Abdominal examination revealed mild hepatosplenomegaly which
confirmed by abdominal US.
• Lymph node examination was normal .
4.
• The patienthad past medical history of infrequent attacks of bronchial
asthma for which he had no chronic medication , and infrequent recurrent
abscesses at different sites of his body
• He is non smoker, non alcoholic and had no chronic drug use
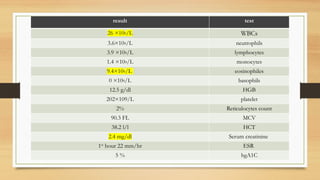
• The patient underwent lab investigations shows the following :
WBCs : arecells of the immune system that are involved in protecting the body
against both infectious disease and foreign invaders
.
Normal Leukocytic count : 4000-11000 per microliter
(
4.5
to 11.0 × 109/L
)
Relative count : relative numbers of each type of WBC in relationship to the
total WBC. It can be expressed as a percentage
Absolute count : the actual number of each cell type (percentage x total
WBC)
.
Ex: if TLC is 4000 with relative neutrophile count 20%
Absolute count will be = (4000 × 20 ) /100 = 800 cells
11.
Differential leukocytic count
Granulocytes: that characterized by
presence of cytoplasmic granules
.
1
-
neutrophiles (polymorphonuclear
leukocytes (PMN) : 50-70%
=
2000-7000
per microliter
2
-
eosinophiles : 1-3%
=
100
-
300
per microliter
3
-
Basophiles : 0.1-1%
=
10-100
per microliter
•
Agranulocyte : lakes of cytoplasmic
granules
.
1
-
lymphocytes : 20-40%
=
1500
-
4000
per microliter
2
-
monocytes : 2%-10%
=
200
-
1000
per microliter
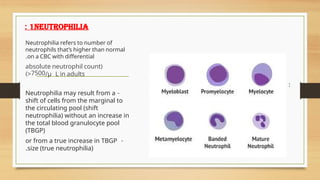
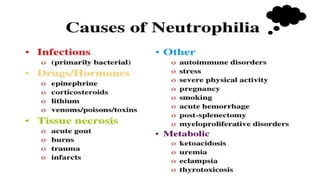
1neutrophilia
:
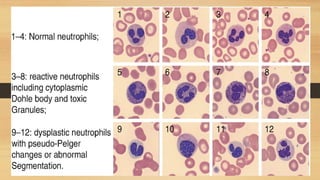
• Normal maturationstages of neutrophils :
Neutrophilia refers to number of
neutrophils that’s higher than normal
on a CBC with differential
.
(
absolute neutrophil count
7500
> /μ L in adults
)
-
Neutrophilia may result from a
shift of cells from the marginal to
the circulating pool (shift
neutrophilia) without an increase in
the total blood granulocyte pool
(TBGP)
-
or from a true increase in TBGP
size (true neutrophilia)
.
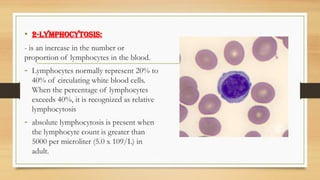
• 2-Lymphocytosis:
- isan increase in the number or
proportion of lymphocytes in the blood.
- Lymphocytes normally represent 20% to
40% of circulating white blood cells.
When the percentage of lymphocytes
exceeds 40%, it is recognized as relative
lymphocytosis
- absolute lymphocytosis is present when
the lymphocyte count is greater than
5000 per microliter (5.0 x 109/L) in
adult.
19.
Types of lymphocytes
:
Blymphocytes make antibodies, which help a person’s
immune system fight pathogens such as bacteria and
viruses
.
T lymphocytes help destroy tumor cells and cells that
are infected with pathogens. They also control the body’s
immune responses
.
Atypical lymphocytes are lymphocytes that activate as
part of the body’s response to infections. They are larger
than normal lymphocytes, with varying sizes and shapes
.
atypical lymphocytes sometimes called “variant
lymphocytes” or “reactive lymphocytes
”.
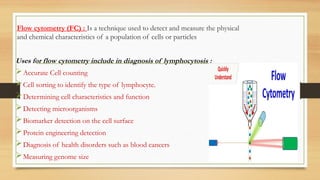
Flow cytometry (FC): Is a technique used to detect and measure the physical
and chemical characteristics of a population of cells or particles
Uses for flow cytometry include in diagnosis of lymphocytosis :
Accurate Cell counting
Cell sorting to identify the type of lymphocyte.
Determining cell characteristics and function
Detecting microorganisms
Biomarker detection on the cell surface
Protein engineering detection
Diagnosis of health disorders such as blood cancers
Measuring genome size
26.
Imaging :
abdominaland neck ultrasound
CT or MRI
Invasive definitive investigations :
Bone marrow Aspirate and biopsy
Lymph node biopsy if accessible .
Investigations for underlying causes:
Autoimmune workup
CRP and PCR for possible infections
Hormonal assessment for possible
Endocrine causes
28.
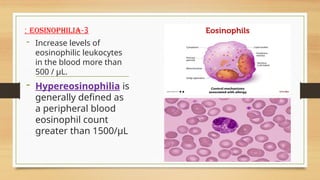
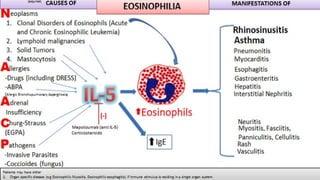
3
-
eosinophilia
:
- Increase levelsof
eosinophilic leukocytes
in the blood more than
500 / μL.
- Hypereosinophilia is
generally defined as
a peripheral blood
eosinophil count
greater than 1500/μL
Careful history taking:
- drug intake
-allergic diseases : asthma or allergic rhinitis and sinusitis
- travel history
Clinical examination for:
-chest disease .
-Cardiac assessment .
-Abdominal examination for organomegaly .
-Skin lesions or change of color .
32.
• Lab investigation:
Stoolanalysis : for parasitic investgaions
CBC with differential leukocytic count
LFT and serum creatinine
Urine analysis for hematuria and urinary eosinophile as; in Churg Strauss and
Wegener's granulomatosis.
• Imaging :
CT chest and abdomen.
Echocardiography.
33.
Bone marrow aspirate:
if persistent eosinophilia more than 3 months
If absolute eosinophilic count more than 1500 per microliter
If no detected secondary cause.
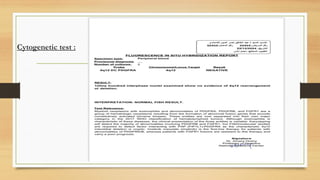
Cytogenetic test :
FISH (fluorescent in situ hybridization) or RT- PCR for detection of
PDGFRA (platelet derived growth factor receptor alpha) mutation
35.
4
-
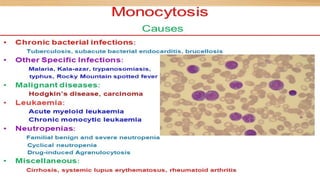
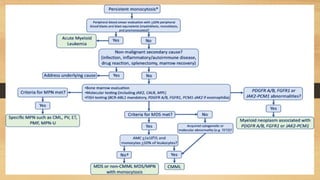
monocytosis
Monocytosis is anincrease in
the number of monocytes
circulating in the blood.
sustained rise in monocyte counts
greater than to 1000/mm3
•Q:other investigations include
•1- stool analysis for parasitic infection ……. Was positive for entamoeba
histolytica and patient received treatment
• 2-Anti bilharzial antibodies …. negative
• 3- live function tests …… was normal
• 4- ANA, p ANCA and c ANCA for exclusion of Wagener granulomatosis and
Churg Strauss …… was negative.
• 5- Serum immunoglobulins to exclude hyper IgE syndrome : showing mild
elevation of serum IgE (253) , with normal IgG.. IgA and IgM levels
45.
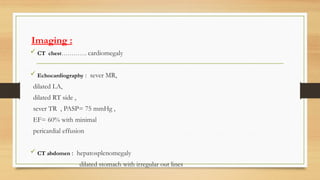
Imaging :
CTchest…………. cardiomegaly
Echocardiography : sever MR,
dilated LA,
dilated RT side ,
sever TR , PASP= 75 mmHg ,
EF= 60% with minimal
pericardial effusion
CT abdomen : hepatosplenomegaly
dilated stomach with irregular out lines




























































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)


