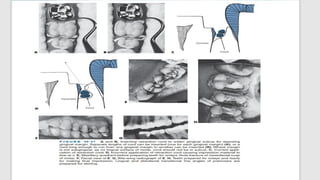
CONVENTIONAL IMPRESSION-Retraction
cord technique
The most common impression materials used for the indirect casting
technique are the polyvinyl siloxanes (addition reaction silicones).
Gingival retraction is to widen the gingival sulcus to provide access for the
impression material to reach the subgingival margins in adequate bulk to
resist tearing during impression withdrawal
Profound local anesthesia substantially reduces salivation to facilitate a dry
field and allows tissue retraction without patient discomfort
4.
Impression
Polyvinyl siloxaneimpressions can withstand disinfection routines without
significant distortion
Two types of trays, commercial stock and custom made, are suitable. Use of
stock, plastic trays is convenient and saves time.
A thickness of impression material greater than 3 mm increases shrinkage and
the chance of voids; a thickness less than 2 mm may lead to distortion or tear
of the impression material
5.
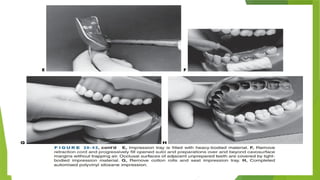
MAKING IMPRESSION
Usethe first dispenser to mix and fill the impression tray with the heavy-bodied impression material .
Now use the second dispenser to mix and inject the light-bodied impression material on the prepared
teeth
The teeth should be examined to ensure that the field is still clean and dry.
. Gently remove the retraction cord with operative pliers.
All preparation surfaces should be clean, dry, and exposed to view.
6.
USE OF LIGHTBODY
Next, deliberately and progressively (moving from distal to mesial) fill the
opened gingival sulci and preparations over and beyond the margins with
material from the syringe.
To avoid trapping air, the tip is kept directly on the gingival and pulpal walls,
filling the preparations from gingival to occlusal, and the flow is regulated so
that material is not extruded too fast ahead of the tip.
Light-bodied material also is injected on the occlusal surfaces of the
unprepared adjacent teeth to eliminate the trapping of air on the occlusal
grooves
7.
REMOVAL OF TRAY
After filling and covering the teeth with material from the syringe,
immediately remove the cotton rolls and seat the loaded tray over the region
After filling and covering the teeth with material from the syringe,
immediately remove the cotton rolls and seat the loaded tray over the region
Removal is aided by inserting a fingertip at the junction of the facial border
of the impression and the vestibule fornix
10.
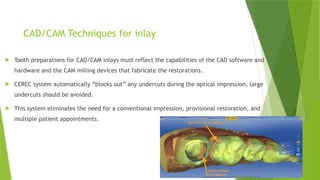
CAD/CAM Techniques forinlay
Tooth preparations for CAD/CAM inlays must reflect the capabilities of the CAD software and
hardware and the CAM milling devices that fabricate the restorations.
CEREC system automatically “blocks out” any undercuts during the optical impression, large
undercuts should be avoided.
This system eliminates the need for a conventional impression, provisional restoration, and
multiple patient appointments.
11.
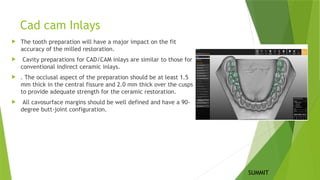
Cad cam Inlays
The tooth preparation will have a major impact on the fit
accuracy of the milled restoration.
Cavity preparations for CAD/CAM inlays are similar to those for
conventional indirect ceramic inlays.
. The occlusal aspect of the preparation should be at least 1.5
mm thick in the central fissure and 2.0 mm thick over the cusps
to provide adequate strength for the ceramic restoration.
All cavosurface margins should be well defined and have a 90-
degree butt-joint configuration.
SUMMIT
12.
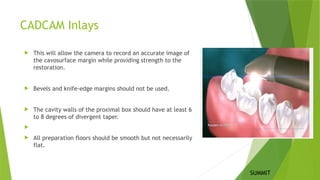
CADCAM Inlays
Thiswill allow the camera to record an accurate image of
the cavosurface margin while providing strength to the
restoration.
Bevels and knife-edge margins should not be used.
The cavity walls of the proximal box should have at least 6
to 8 degrees of divergent taper.
All preparation floors should be smooth but not necessarily
flat.
SUMMIT
Metal CERAMIC composite
INDICATIONS
1..Extensive tooth loss, Correction
of occlusion
2. Large class 2
3. Restoration of endodontically
treated teeth
4. Longevity and durability
5. Preexisting cast metal
restorations
CONTRAINDICATIONS
6. Occlusal disharmony
7. Aesthetics
1.ESTHETICS
2.Moderate sized cavities
3]When precise fit and strength needed
1]Heavy occlusal forces
2] Inability to maintain a dry field.
3] Deep subgingival preparation.
1.ESTHETICS
2. WORN-OUT TOOTH
3]Limited occlusal stresses
4]Isolation
1]BRUXISM
2]ALLERGY
18.
Metal CERAMIC composite
ADVANTAGES
1.Greatertensile strength
2.Precise reproduction of the form
and minute details
3.Metal alloys used are tarnish and
corrosion resistant
4. Finishing and polishing can be
done outside the oral cavity, thus
preventing damage to the pulp
DISADVANTAGES
1. Leakage around and under the
restorations through the
cement- restoration - tooth
junction
2.It involves extensive tooth
preparation
3.Technique sensitive
4. Galvanic deterioration
1]Wear resistance—Ceramic
restorations are more wear
resistant than direct composite
restorations.
Ability to strengthen remaining
tooth structure
3]More precise control of contours
and contacts
4]Biocompatibility and good tissue
response
1]Brittleness of ceramics.
2]Wear of opposing dentition and
restoration.
4]Low potential for repair
1]Bonding and reinforcement
2]Reduced sensitivity
3]Repairability
4]Conservative tooth preparation
5]Biocompatibility
1]Durability
2]Staining and discolouration
3]less lifespan
4]technique sensitive
5]limited strength in large
restorations
19.
Cast gold usuallymade of
copper, silver, platinum, nickel,
zinc
Gold offers high strength and
durability.
They are more suitable for
posterior teeth where
esthetics are not a primary
concern
Ceramic restorations, also
known as porcelain
restorations, are made of
dental-grade ceramic
materials.
They are generally not as
strong as metal restorations.
They are highly esthetic and
are commonly used in the
front teeth.
Resin composite restorations
are made of a mixture of
plastic (composite resin) and
fine glass particles
They are generally not as
strong as ceramics or metals.
They offer excellent esthetics
and are commonly used in
both front and back teeth.
Metal CERAMIC composite
LUTING CEMENT:
Zinc phosphate cement provides
good retention and is particularly
useful for cast gold restorations
due to its ability to bond to both
metal and tooth
structure[Donovan and Cho, 1999]
TOOTH PREPERATION:
Bevel is needed
For Metal inlays, a slight
divergence or taper of 2 to 5
degrees is required
Occlusal Reduction:1-1.5 mm
Resin cements are widely used for
luting ceramic restorations due to
their excellent adhesive properties
and esthetics
Bevel is usually not recommended
The divergence angle of more
than[ 2 to 5]. helps ensure a
secure fit and stability of the
restoration within the tooth
preparation
1.5 to 2mm.
Resin cements used for composite
inlays are typically dual-cured or
light-cured
[el-Mowafy et al. ]
Bevel not needed.
The divergence angle of [more
than 2 to 5 degrees] same as
ceramic
1.5 to 2mm
20.
Cast gold CERAMICcomposite
Biocompatibility is good
ADAPTABILITY
Gold restorations are more
adaptable
LONGEVITY
Metal restorations known for
their durability [Leempoel et al. ]
TYPE OF TOOTH PREP
Metal restorations usually require
less tooth removal compared to
ceramics
Dental ceramics are generally
biocompatible
Ceramics are difficult to adapt
Ceramic restorations are known
for their excellent long-term
durability[Wendt SL etal]
Ceramic restorations may
require more tooth structure
removal
They are also biocompatible
Composites are also difficult to
adapt
They tend to have a shorter
lifespan compared to ceramic
restorations. [Taylor DF, et al]
Resin composite restorations
require less tooth structure
removal
21.
Cast gold CERAMICcomposite
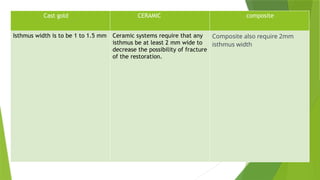
Isthmus width is to be 1 to 1.5 mm Ceramic systems require that any
isthmus be at least 2 mm wide to
decrease the possibility of fracture
of the restoration.
Composite also require 2mm
isthmus width
Feature Direct InlayIndirect Inlay
Visits Required One Two or more
Material Strength Moderate High (ceramic, gold, etc.)
Fit Accuracy Moderate Excellent
Aesthetic Options Good (composite) Excellent (porcelain/zirconia)
Cost Lower Higher
Durability Fair to good Excellent
Technique Chairside, fast Lab/CAD-CAM-based
Ideal Use Small to moderate restorations
Larger restorations or high stress
areas
29.
CAD/CAM
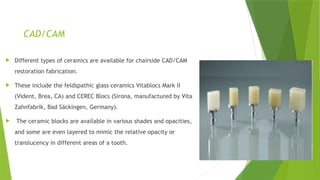
Different typesof ceramics are available for chairside CAD/CAM
restoration fabrication.
These include the feldspathic glass ceramics Vitablocs Mark II
(Vident, Brea, CA) and CEREC Blocs (Sirona, manufactured by Vita
Zahnfabrik, Bad Säckingen, Germany).
The ceramic blocks are available in various shades and opacities,
and some are even layered to mimic the relative opacity or
translucency in different areas of a tooth.
30.
Impression
Gingival retractioncord can be used to reflect the gingival tissues away from the tooth structure thus
providing access to the impression material to reach the subgingival margins.
Tooth-colored inlay systems require an elastomeric or optical impression of the prepared tooth and the
adjacent teeth and interocclusal records, which allow the restoration to be fabricated on a working
cast in the laboratory.
With chairside CAD/CAM systems, no working cast is necessary.
31.
CAD/CAM
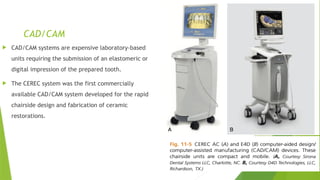
CAD/CAM systemsare expensive laboratory-based
units requiring the submission of an elastomeric or
digital impression of the prepared tooth.
The CEREC system was the first commercially
available CAD/CAM system developed for the rapid
chairside design and fabrication of ceramic
restorations.





![Metal CERAMIC composite
INDICATIONS
1. .Extensive tooth loss, Correction
of occlusion
2. Large class 2
3. Restoration of endodontically
treated teeth
4. Longevity and durability
5. Preexisting cast metal
restorations
CONTRAINDICATIONS
6. Occlusal disharmony
7. Aesthetics
1.ESTHETICS
2.Moderate sized cavities
3]When precise fit and strength needed
1]Heavy occlusal forces
2] Inability to maintain a dry field.
3] Deep subgingival preparation.
1.ESTHETICS
2. WORN-OUT TOOTH
3]Limited occlusal stresses
4]Isolation
1]BRUXISM
2]ALLERGY](https://image.slidesharecdn.com/inlayautosaved-250714163135-b47448e9/85/DIFFERENT-TYPES-OF-INLAY-COMPARISON-AND-IMPRESSION-MAKING-17-320.jpg)
![Metal CERAMIC composite
ADVANTAGES
1.Greater tensile strength
2.Precise reproduction of the form
and minute details
3.Metal alloys used are tarnish and
corrosion resistant
4. Finishing and polishing can be
done outside the oral cavity, thus
preventing damage to the pulp
DISADVANTAGES
1. Leakage around and under the
restorations through the
cement- restoration - tooth
junction
2.It involves extensive tooth
preparation
3.Technique sensitive
4. Galvanic deterioration
1]Wear resistance—Ceramic
restorations are more wear
resistant than direct composite
restorations.
Ability to strengthen remaining
tooth structure
3]More precise control of contours
and contacts
4]Biocompatibility and good tissue
response
1]Brittleness of ceramics.
2]Wear of opposing dentition and
restoration.
4]Low potential for repair
1]Bonding and reinforcement
2]Reduced sensitivity
3]Repairability
4]Conservative tooth preparation
5]Biocompatibility
1]Durability
2]Staining and discolouration
3]less lifespan
4]technique sensitive
5]limited strength in large
restorations](https://image.slidesharecdn.com/inlayautosaved-250714163135-b47448e9/85/DIFFERENT-TYPES-OF-INLAY-COMPARISON-AND-IMPRESSION-MAKING-18-320.jpg)
![Cast gold usually made of
copper, silver, platinum, nickel,
zinc
Gold offers high strength and
durability.
They are more suitable for
posterior teeth where
esthetics are not a primary
concern
Ceramic restorations, also
known as porcelain
restorations, are made of
dental-grade ceramic
materials.
They are generally not as
strong as metal restorations.
They are highly esthetic and
are commonly used in the
front teeth.
Resin composite restorations
are made of a mixture of
plastic (composite resin) and
fine glass particles
They are generally not as
strong as ceramics or metals.
They offer excellent esthetics
and are commonly used in
both front and back teeth.
Metal CERAMIC composite
LUTING CEMENT:
Zinc phosphate cement provides
good retention and is particularly
useful for cast gold restorations
due to its ability to bond to both
metal and tooth
structure[Donovan and Cho, 1999]
TOOTH PREPERATION:
Bevel is needed
For Metal inlays, a slight
divergence or taper of 2 to 5
degrees is required
Occlusal Reduction:1-1.5 mm
Resin cements are widely used for
luting ceramic restorations due to
their excellent adhesive properties
and esthetics
Bevel is usually not recommended
The divergence angle of more
than[ 2 to 5]. helps ensure a
secure fit and stability of the
restoration within the tooth
preparation
1.5 to 2mm.
Resin cements used for composite
inlays are typically dual-cured or
light-cured
[el-Mowafy et al. ]
Bevel not needed.
The divergence angle of [more
than 2 to 5 degrees] same as
ceramic
1.5 to 2mm](https://image.slidesharecdn.com/inlayautosaved-250714163135-b47448e9/85/DIFFERENT-TYPES-OF-INLAY-COMPARISON-AND-IMPRESSION-MAKING-19-320.jpg)
![Cast gold CERAMIC composite
Biocompatibility is good
ADAPTABILITY
Gold restorations are more
adaptable
LONGEVITY
Metal restorations known for
their durability [Leempoel et al. ]
TYPE OF TOOTH PREP
Metal restorations usually require
less tooth removal compared to
ceramics
Dental ceramics are generally
biocompatible
Ceramics are difficult to adapt
Ceramic restorations are known
for their excellent long-term
durability[Wendt SL etal]
Ceramic restorations may
require more tooth structure
removal
They are also biocompatible
Composites are also difficult to
adapt
They tend to have a shorter
lifespan compared to ceramic
restorations. [Taylor DF, et al]
Resin composite restorations
require less tooth structure
removal](https://image.slidesharecdn.com/inlayautosaved-250714163135-b47448e9/85/DIFFERENT-TYPES-OF-INLAY-COMPARISON-AND-IMPRESSION-MAKING-20-320.jpg)














































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

