2
• Title: Clinicalperformance of Direct verses Indirect Composite Restorations
in posterior teeth: A Systematic Review
• Case report: Esthetic Restoration of Mandibular Molar by Indirect Composite
Restoration with Cusp Capping.
• Name of Presenter: Dr. Avneet Kaur
• Department: Department of Conservative Dentistry and Endodontics
MAHATMA GANDHI DENTAL COLLEGE & HOSPITAL
A unit of Mahatma Gandhi University of Medical Sciences & Technology
4
Introduction
Today’s dental patientconcerned about attractive restorations is looking
for a dentist who incorporates the newest and best techniques into
practice
In the past 5 years, many types of tooth colored inlays and onlays
have been introduced to the profession
Evolution of esthetic dentistry persist through innovations in
bonding agents, restorative materials, and conservative
preparation techniques
5.
5
• Patients’ concernfor esthetic appearance, and dentists’ appreciation of the
additional strength of the restored tooth from acid etching and bonding have
generated interest in these restorations
6.
6
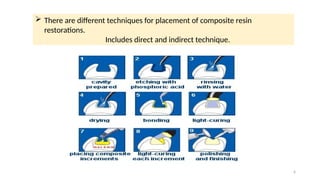
There aredifferent techniques for placement of composite resin
restorations.
Includes direct and indirect technique.
8
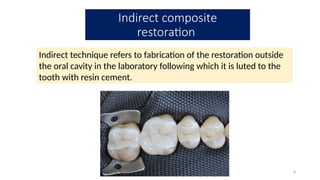
Indirect technique refersto fabrication of the restoration outside
the oral cavity in the laboratory following which it is luted to the
tooth with resin cement.
Indirect composite
restoration
9.
9
Definition
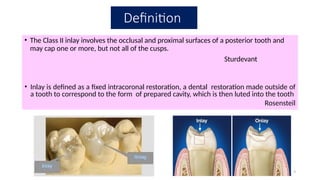
• The ClassII inlay involves the occlusal and proximal surfaces of a posterior tooth and
may cap one or more, but not all of the cusps.
Sturdevant
• Inlay is defined as a fixed intracoronal restoration, a dental restoration made outside of
a tooth to correspond to the form of prepared cavity, which is then luted into the tooth
Rosensteil
10.
10
Classification Based onEvolution
First generation
Introduced in the early 1980.
These materials were developed in an attempt to overcome the
polymerization shrinkage and wear seen with direct composite
restorations.
But these also had poor physical properties because of low filler
and high matrix load.
Flexural strength (60–80
MPa)
Elastic modulus (2–3.5 GPa)
Resin volume more than 50%
11.
11
It was observedthat the degree of conversion
increased up to 44%.
It was observed that supplementing conventional
photo-cure with additional cure increased monomer
conversion but did not improve physical properties.
J Conserv Dent. 2010 Oct-Dec;
13(4): 184–194.
12.
12
Second generation: theywere introduced after mid 1990s so as
to have better properties than first generation indirect
restorations. which included microhybrid composites with fillers
of approximately 66% by volume.
This resulted in improved mechanical properties with flexural
strength in the range of 120–160 MPa and elastic modulus of
8.5–12 GPa.
Structure and composition
14
Thesecond-generation composites have filler with a diameter
of 0.04–1 µ.
By increasing the filler load, the mechanical properties and
wear resistance improved.
The new composite resins like Artglass® and belleGlass HP®
contain high amounts of filler content, which make them
adequate for restoring posterior teeth.
15.
Polymerization techniques
15
Light curingextra-orally did not efficiently improve
the degree of conversion.
Thus, specific conditions like heat, vacuum, pressure,
and oxygen-free environment are utilized for
polymerization of second-generation IRCs.
Ferracane JL, Condon JR. Post-cure heat
treatments for composites: Properties and
fractography. Dent Mater. 1992;8:290–5
16.
Heat
16
• Temperature usuallyused for IRC ranges from 120–140°C.
• This concept was first used by Heraeus-Kulzer.
• It was observed that the wear resistance increased by 35% on curing
with both light and heat when compared to curing with light only.
Nitrogen atmosphere
• Nitrogen pressure eliminates internal oxygen before the material
begins to cure.
• This influences the degree of conversion, esthetics, wear, and
abrasion.
17.
• Belle glassHP
• Microhybrid composite having cured at a temperature of 138’C under 29 psi
pressure in nitrogen environment.
• high flexural and compressive strengths,
• Thus it can be an ideal material in cases of high occlusal forces.
• Variety of colors are available in this system .
The available commercial system for
fabrication
17
• Art Glass
• Microhybrid polymer glass material having 78% inorganic filler
by weight.
• Having a 4-6 functional groups.
• More double bond conversion and increase cross linking.
• These are specially cured with xenon-stroboscopic light 320-
500nm
18.
18
Advantages
Improved physical properties
Wearresistance
More precise control of contours and contacts
Reduced polymerization shrinkage
Ability to strengthen remaining tooth structure
Biocompatibility and good tissue response
19.
19
DISADVANTAGES
Increased cost andtime
Technique sensitivity
Requires two appointments
Wear of opposing dentition and restorations
Resin-to-resin bonding difficulties
Low potential for repair
Difficult intraoral polishing
22
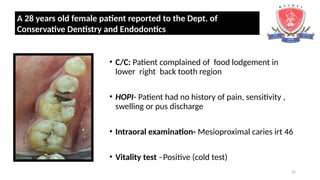
• C/C: Patientcomplained of food lodgement in
lower right back tooth region
• HOPI- Patient had no history of pain, sensitivity ,
swelling or pus discharge
• Intraoral examination- Mesioproximal caries irt 46
• Vitality test –Positive (cold test)
A 28 years old female patient reported to the Dept. of
Conservative Dentistry and Endodontics
23.
23
• Radiographic Examination: Radiolucency involving
coronal to middle one-third involving enamel and dentin
in mesioproximal region suggestive of mesioproximal
caries irt #46
• Diagnosis – class II (mesioproximal caries )irt 46
• Treatment plan – Indirect Restoration irt 46
Composite Inlay Ceramic Inlay
27
Tooth preparation
• No.271 - Aid in development of
uniformly tapered walls
• Sides and end surface of the No. 271 bur
meet in a slightly rounded manner so that
sharp, stress-inducing internal angles will
not be formed in the preparation.
Armamentaria
28.
28
No. 169L -Dovetail Retention , Retention Grooves
No. 8862 - Development of marginal bevels and
secondary flares
Carbide bur or diamond
tapering instrument that
creates occlusally divergent
facial and lingual walls for
ceramic inlays.
29.
29
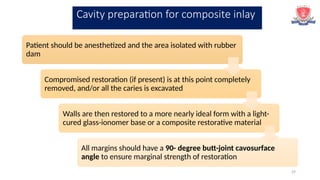
Patient should beanesthetized and the area isolated with rubber
dam
Compromised restoration (if present) is at this point completely
removed, and/or all the caries is excavated
Walls are then restored to a more nearly ideal form with a light-
cured glass-ionomer base or a composite restorative material
All margins should have a 90- degree butt-joint cavosurface
angle to ensure marginal strength of restoration
Cavity preparation for composite inlay
30.
30
Initial cavitypreparation should be done with the flat end tapered
carbide bur
This result in facial and lingual walls that diverge occlusally
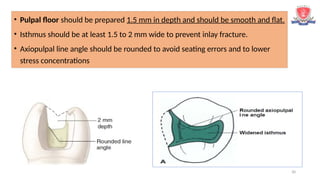
• Pulpal floor should be prepared 1.5 mm in depth and should be smooth and flat.
• Isthmus should be at least 1.5 to 2 mm wide to prevent inlay fracture.
• Axiopulpal line angle should be rounded to avoid seating errors and to lower
stress concentrations
31.
31
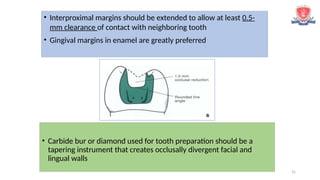
• Interproximal marginsshould be extended to allow at least 0.5-
mm clearance of contact with neighboring tooth
• Gingival margins in enamel are greatly preferred
• Carbide bur or diamond used for tooth preparation should be a
tapering instrument that creates occlusally divergent facial and
lingual walls
32.
32
Junction of thesides and tip of
the cutting instrument should
have a rounded design to avoid
creating sharp, stress-inducing
internal angles in preparation
2° to 5° per wall recommended
for cast metal inlays and onlays-
Divergence can be increased
because the tooth colored
restoration will be adhesively
bonded and because very little
pressure can be applied during
try-in and cementation
33.
33
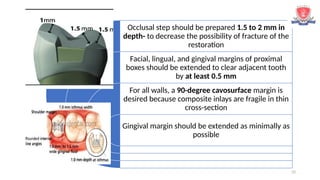
Occlusal step shouldbe prepared 1.5 to 2 mm in
depth- to decrease the possibility of fracture of the
restoration
Facial, lingual, and gingival margins of proximal
boxes should be extended to clear adjacent tooth
by at least 0.5 mm
For all walls, a 90-degree cavosurface margin is
desired because composite inlays are fragile in thin
cross-section
Gingival margin should be extended as minimally as
possible
34.
34
Bevels are contra-indicatedbecause composite are brittle
and thin knife edge margins may easily fracture under
occlusal forces
Another school of thought advocates that placement of
hollow ground chamfer is preferable because it provides
more area for etching and hence better seal is achieved as
well as it improves aesthetic colour blending.
35.
35
Cusp capping
• Whena portion of facial or lingual surface is affected by caries
or other defect, it may be necessary to extend preparation
around the transitional line angle to include the defect
• When extending through or along cuspal inclines to reach sound
tooth structure, a cusp usually should be capped if the extension is
two thirds or greater than distance from any primary groove to the
cusp tip
36.
36
• Centric holdingcusps capping- Necessary to prepare a shoulder to
move facial or lingual cavosurface margin away from any possible
contact with opposing tooth, during functional movements
If cusps must be capped, they should be reduced 1.5 to 2 mm and
should have a 90- degree cavosurface angle.
Such contacts directly on margins can
lead to premature deterioration of
marginal integrity
• The axial wall of the resulting shoulder: deep to allow for adequate thickness of
restorative material
• Should have same path of draw as the main portion of preparation
37.
37
A provisional ortemporary restoration is necessary when
using indirect systems that require two appointments.
Direct Technique
Indirect Technique
Provisional Restoration
38.
38
Place in thecavity with light pressure
Overcontoured proximal surfaces will
block the fit- then recontour
With mouth mirror evaluate the
fit
Use a floss at contacts to evaluate
tightness and position
Use Abrasive disks to adjust proximal
contour
Try-in and Cementation
39.
39
Indirect composite restorationsare
bonded to tooth structure by :
Etching enamel to increase the
bondable surface area
Etching, priming, and applying the bonding
agent to dentin (when appropriate)
Etching (by hydrofluoric acid) and then
priming (silanating) the restoration
cementing the restoration with composite
cement(resin)
Applying hydrofluoric acid for 2min
to internal surface of composite
inlay. After rinsing and drying, etched
surfaces should have a "frosty" white
appearance.
Bonding and cementation of indirect composite
restoration
40.
40
A dual-cure compositecement is inserted into the preparation
and internal surfaces of the restoration
The inlay is immediately inserted into the prepared tooth,
using light pressure.
A ball burnisher applied with a slight vibrating motion is used
to seat the restoration
Excess composite cement is removed and light-cured 60
seconds in each direction
41.
41
• For indirectcomposite restorations, finishing may be started with 12-fluted
carbide finishing burs instead of diamonds.
• Interproximally, a No. 12 surgical blade: remove excess composite cement
when access permits
• Abrasive strips of successively finer grits: to remove slight interproximal
excesses
Finishing of indirect composite restoration
42.
42
• Slender flameshapes are used interproximally, while larger oval
or cylindric shapes are used on the occlusal surface
• 30-fluted carbide finishing burs are used to obtain a smoother
finish
43.
43
• The studyconcluded that indirect restorations have less surface roughness,
postoperative sensitivity, and soft-tissue irritation than direct restorations. The
clinical performances of the indirect restorations were more satisfactory than the
direct restorations.
Duke et al reached a 70.7% success rate 36 months after
placement and concluded that indirect composite resin
restorations represent a good choice for the therapy of severely
damaged teeth.
44.
44
Indirect composite restorationshave superior surface texture, anatomic
form, occlusion, tooth integrity, lesser sensitivity and marginal
discoloration whereas direct composite restorstions have shown superior
restorstion integrity.
45.
45
Advances in composite,and adhesive technology have resulted in the
development of a variety of tooth-colored indirect restorations
These offer an excellent alternative to direct composite restorations, especially for
large restorations, and are more conservative than full-coverage restorations
However, because the clinical procedures are relatively technique-sensitive,
proper case selection, operator skill, and attention to detail are critical to success.
Conclusion
#6 Single visit direct composite restorations allows for preservation of tooth structure.In this technique, following etching and application of bonding agent to the prepared cavity, composite restoration is built up in increments, curing one layer at a time. Hence, cavities are filled incrementally with facially and lingually inclined mesiodistal layers of maximum 2 mm
#7 Advantages of direct technique include increased
#10 In spite of their secondary curing, they exhibited low levels of flexural strength (60–80 MPa) and elastic modulus (2–3.5 GPa), a resin volume more than 50% and higher wear levels.[6
#11 Conversion of monomeric c-c double bond into polymeric c-c single bond
#18 Indirect comp rest r more wear resistant than direct composite
#19 ceramic restoration can fracture if the preparation does not provide adequate thickness to resist occlusal forces a
Laboratory-processed composites are highly cross-linked, so few double bonds remain available for chemical adhesion of the composite cement . 44 Therefore the composite restoration must be mechanically abraded and/or chemically treated to facilitate adhesion of the cement
#21 Margins are difficult to record with an impression and are difficult to finish. Additionally, bonding to enamel margins is greatly preferred, especially along gingival margins of proximal boxes.
#23 Based on clinical examination ,as the caries portion involves more than 2/3 of lingual cusp ,the treatment plan indirect restoration that inlay with cusp capping was made pt was explained about the restoration either with composite and cermic, and due to financial reasons pt chose