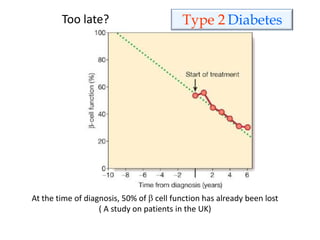
Downloaded 1,161 times
![Classification of diabetes
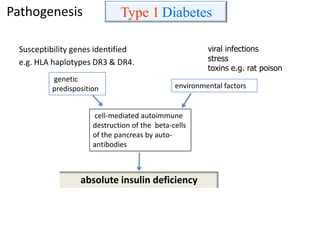
Type 1 ( was called “insulin- dependent DM”/ juvenile type of DM) ( 5-10%)
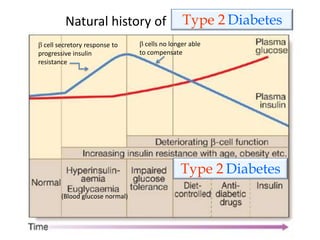
Type 2 (was called “non insulin- dependent DM” /adult onset DM ) (90-95%)
The “pre-diabetic stage” (impaired glucose tolerance)
Gestational DM -any degree of glucose intolerance with onset or first
recognition during pregnancy [in 2-5% of all pregnancies]
Other specific types (1% - 2%)
– genetic syndromes (affecting insulin secretion or action)
– endocrinopathies (Acromegaly, Cushing’s syndrome, glucagonoma,
pheochromocytoma, thyrotoxicosis)
– diseases of pancreas (chronic pancreatitis, cancer)
– drug- or chemical-induced (corticosteroids, beta-blockers, thiazide
diuretics)
– infections (viral)
The main focus of this plenary](https://image.slidesharecdn.com/diabetesmellitus-pathophysiol-vnw-130817094220-phpapp01/85/Diabetes-mellitus-pathophysiol-vnw-5-320.jpg)
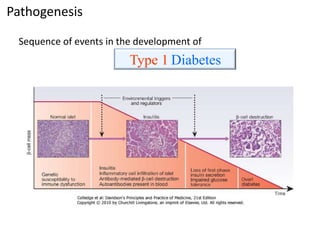
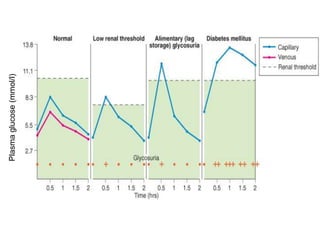
![(1) Symptoms (thirst, increased urination,
unexplained weight loss) + a random plasma glucose
concentration >200 mg/dL (11.1 mmol/L).
(2) Fasting plasma glucose (FPG) >126 mg/dL (7.0
mmol/L) after an overnight (at least 8-hour) fast
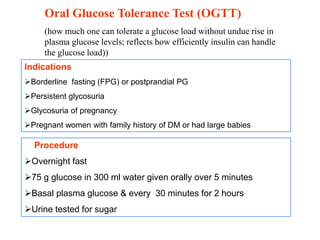
(3) Two-hour plasma glucose greater than 200 mg/dL
(11.1 mmol/L) during a standard 75-g oral glucose
tolerance test (OGTT)
[ should be confirmed on a later day with one of the
three methods listed]](https://image.slidesharecdn.com/diabetesmellitus-pathophysiol-vnw-130817094220-phpapp01/85/Diabetes-mellitus-pathophysiol-vnw-33-320.jpg)

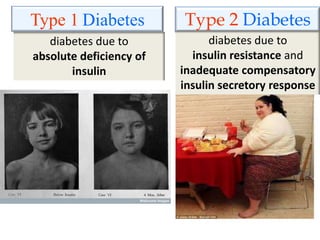
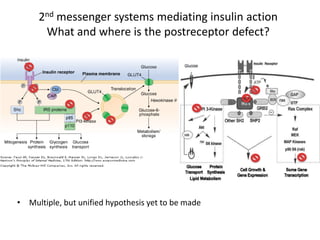
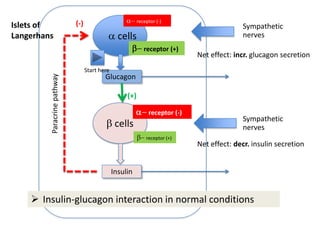
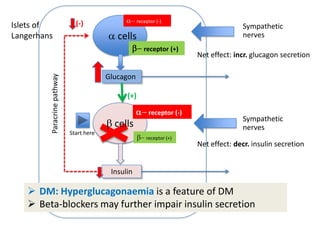
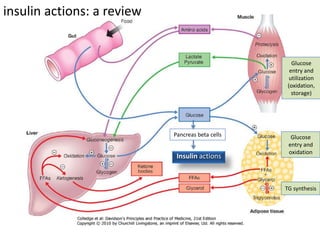
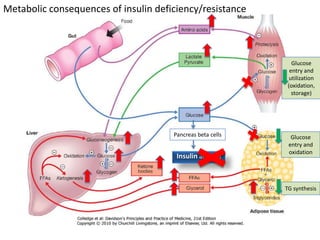
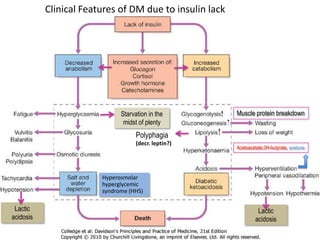
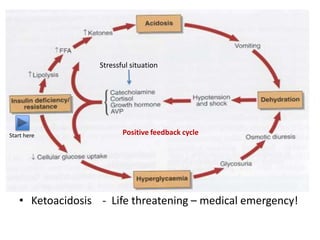
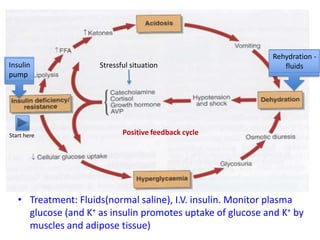
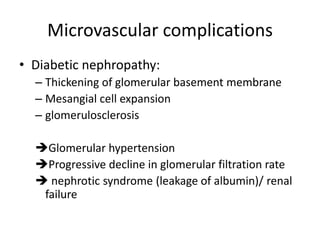
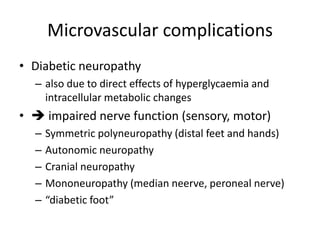
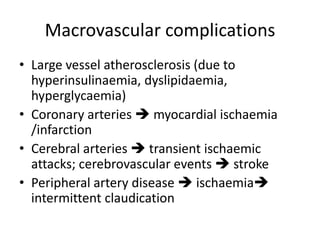
This document discusses diabetes mellitus and its various types and complications. It defines diabetes as a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion or insulin action. There are two main types - type 1 diabetes which results from an absolute deficiency of insulin due to autoimmune destruction of pancreatic beta cells, and type 2 diabetes which is due to insulin resistance and inadequate insulin secretion. The document outlines the pathogenesis, clinical presentation, diagnostic criteria and long term complications of both types of diabetes, which can include damage to blood vessels, nerves, eyes and kidneys if not properly managed.












































































