This document outlines requirements and procedures for Child Protective Services regarding family preservation and conducting Comprehensive Child and Family Assessments (CCFAs). It states that DFCS must initiate a CCFA within 1 day of a preliminary protective hearing and collaborate with Amerigroup to ensure children receive medical exams. It provides details on the components that must be included in CCFAs and the process that DFCS and providers must follow to complete them.











































![Child Protective Services: Family Preservation
Social Services Manual Child Protective Chapter 2100, Section VII
September 2000 Page 128
Assessment, by identifying persons or agencies that will take responsibility for a child’s
safety. It provides a detailed description of the specific steps that everyone participating
in the plan has agreed to for keeping a child safe. A safety plan is completed for every
substantiated report and for any unsubstantiated case that is required to remain open
(e.g. court-ordered supervision). A plan is completed at any time during an investigation
that a safety assessment suggests a child might not be safe. There must be a plan in
place by the completion of the investigation on substantiated reports and those
that will remain open for court-ordered supervision.
One safety plan can be developed for all children in the family; however, it must be
individualized, as needed, to cover the conditional and unique safety needs of any child
whose needs differ from needs of other children covered by the plan.
Remember, Form 455B (Safety Plan) is not a case plan. The case plan identifies
selected goals and the steps to be followed when making the long-term changes
necessary for future and ongoing protection and safety of a child. The Safety Plan
describes the safety controls that are in place up until the time a case plan is
developed and activated. However, a new safety plan may be needed whenever
circumstances change and a new safety assessment determines that new controls are
needed to ensure safety. A Safety Plan remains in place while the ongoing case
manager assesses the family’s strengths and needs and develops with the family
a case plan. The ongoing case manager who receives a case in transfer from
investigations must continue to follow the safety plan, as written, or work with the
involved parties of the plan to make any needed adjustments.
Requirement
Complete a Safety Plan*, using Form 455B, for:
Any child with substantiated maltreatment;
Any child whose circumstances require a safety plan prior to the investigation
being completed;
Any child in an unsubstantiated case that is required to remain open:
Any child in an ongoing CPS case when a reassessment indicates risk level has
increased, or as needed when safety concerns are identified.
*[Exception: a safety assessment and safety plan are not completed when the alleged
maltreater is a day care provider, foster parent, school employee or an agency standing
in loco parentis.]
The Safety Plan requires a response for each identified behavior or condition (safety
factors) answered with a “Yes” on the Safety Assessment. Restate each Safety Factor
on the Safety Plan. Involve parents and others who will be responsible for a child’s care
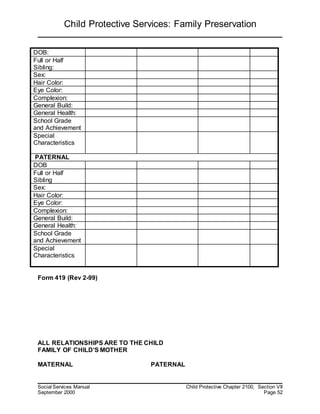
with the development of the safety plan. Include the following information:](https://image.slidesharecdn.com/dfcsdocsimportant04112015-150714130648-lva1-app6891/85/Dfcs-docs-important-04112015-128-320.jpg)



![Page144 of 306
stringent standard of proof necessary to modify a custody award. In the Interest of W.W.W., 213 Ga. App.
732 (1994). All deprivation proceedings arising between the child's parents must be originally filed in
superior court. If the superior court judge determines that the deprivation proceeding is not a custody
dispute in disguise, the judge will transfer the deprivation issues to the juvenile court for adjudication. In
the Interest of M.A. et al., Children, 218 Ga. App. 433 (1995). Thus, during the investigation of an
allegation of deprivation, it is possible that the caseworker will have some contact with the superior court
system as well.
[Juv-Sup Graphic Goes Here]
B. Definition of Deprivation
The code lists four circumstances in which a child can be considered "deprived". When the child:
1. is without proper parental care or control, subsistence, education as required by law, or other
care or control necessary for his physical, mental, or emotional health or morals;
2. has been placed for care or adoption in violation of the law;
3. has been abandoned by his parents or other legal custodian; or
4. is without a parent, guardian, or custodian.
O.C.G.A. § 15-11-2(8)(A-D).
One important exception is specifically listed in the code. "No child who in good faith is being treated solely](https://image.slidesharecdn.com/dfcsdocsimportant04112015-150714130648-lva1-app6891/85/Dfcs-docs-important-04112015-144-320.jpg)



![Page148 of 306
deceased and another is incarcerated. In re J.R.T., a Child, 233 Ga. 204 (1974). However, given the large
number of deprivation cases involving incarcerated parents that are filed under the general category of a
"lack of parental care or control" it seems clear that this category is rarely used for that purpose.
[Deprivation Graphic Goes Here]
C. Venue
The SAAG representing your county must now consider in which juvenile court to file a deprivation petition.
This decision is called venue. A deprivation proceeding may be commenced in any county in which the child
resides or in any county where the child is present when action was taken to protect the child. O.C.G.A. §
15-11-29(a). If your county has either a full or part time juvenile court judge to hear deprivation cases, the
hearing should occur in your county since that will be where either the child resides or where the child was
present when the legal action was commenced. If your county has a superior court judge who periodically
hears juvenile court cases, the superior court judge can choose to hear your case in any county within your
judicial circuit. O.C.G.A. § 15-11-29(b). In such situations, it may be necessary for you to travel to another
county to appear in a deprivation hearing.
[Deprivation Flow Chart Goes Here.]
III. Removing A Deprived Child From The Home
A. Protective Custody](https://image.slidesharecdn.com/dfcsdocsimportant04112015-150714130648-lva1-app6891/85/Dfcs-docs-important-04112015-148-320.jpg)


![Page151 of 306
[Removing Child from the Home Graphic Goes Here.]
IV. 72-Hour Informal Detention Hearing
A. When is the hearing required? What must be shown?
An informal detention hearing within 72 hours of the child's removal from the home is required when the
juvenile court or the court intake officer has not released the child to the custody of his or her parents after
removal from the home. If the 72-hour period expires on a Saturday, Sunday, or legal holiday, the hearing
must be held on the next day of business which is not a Saturday, Sunday, or legal holiday. O.C.G.A. § 15-
11-49(c)(3). The Georgia Supreme Court has interpreted this time frame to be mandatory and if the hearing
is not held within 72 hours of the child's removal, the deprivation action should be dismissed without
prejudice. Sanchez v. Walker Co. Dept. of Family and Children Services, 237 Ga. 406 (1976). Dismissal
"without prejudice" means that the department may refile a deprivation petition if it has reason to believe
that the child is abused or neglected. It would seem that a dismissal of a petition would require returning a
child to the custody of his/her parent(s). However, given the court's authority to issue preliminary protective
custody orders based on allegations contained in a petition, there seems to be nothing to prevent a juvenile
court judge from issuing another "pick up" order to again detain the child should the court feel that the
situation warrants such action. If a parent fails to make a timely objection during the informal detention
hearing that the statutory time limits have not been observed, this objection is effectively waived and
cannot be raised on appeal. Irvin v. Department of Human Resources, 159 Ga. App. 101 (1981). While the
procedure allows the case to go forward, the delay associated with beginning the process over again is
burdensome for the DFCS caseworker and may result in either returning a child into a potentially harmful
home environment or extending the time a child will spend in shelter care. Adequate preparation to make
sure that both the SAAG and DFCS caseworker are prepared and ready for the informal detention hearing is
essential.
At the 72-hour hearing, the judge will determine if it is safe to return the child or if the child should be
detained until a full hearing can be held to determine whether the child is deprived. The hearing provides
the child's parents with judicial review of the actions taken by the juvenile court intake officer. Most juvenile
courts have interpreted the 72-hour hearing as the equivalent of a probable cause hearing which uses a
standard of proof known as preponderance of the evidence. The petitioner must show evidence to indicate
that it is "more likely than not" that the child is deprived. This is a much lower burden of proof on DFCS than
will be required at the formal adjudicatory hearing (trial) on the merits of the deprivation petition.
Remember, if the juvenile court intake officer released the child to the custody of his/her parents, it will not
be necessary to hold a 72-hour hearing prior to the adjudicatory hearing if DFCS determines to pursue the
matter further.
The person who represents the petitioner in the 72-hour informal detention hearing varies from jurisdiction](https://image.slidesharecdn.com/dfcsdocsimportant04112015-150714130648-lva1-app6891/85/Dfcs-docs-important-04112015-151-320.jpg)


![Page154 of 306
child was in effect made a party to the proceeding and therefore had standing to appeal the judgement
through the GAL. Miller v. Rieser, 213 Ga. App. 683 (1994). The court came to a similar conclusion in a
proceeding to terminate parental rights where the statute mandates the appointment of a guardian ad
litem. In re G.K.J., 187 Ga. App. 443 (1988).
If the child is old enough to have some understanding of the proceedings, the guardian ad litem will need to
explain the court process to the child and make
sure that the child's wishes are known to the court. Ferreira, McGough's Juvenile Practice and Procedure
(2nd ed), at § 4-14. However, under Ethical Considerations 7-12 and 7-17 of the Code of Professional
Responsibility, an attorney acting as a guardian ad litem is not required to change his/her recommendation
to the court based upon the wishes of the child. The GAL's role in the deprivation process is to make a
recommendation in the best interests of the child which may mean a recommendation that is contrary to
what the child desires. Id. at § 4-14. This differs from the role of an attorney in other proceedings to
advocate for the position of his/her client. Some believe that a conflict of interest could develop in a
situation where an attorney serves as both as the child's counsel (advocate) as well as guardian ad litem
and the attorney's recommendation differs from the wishes of the child. The Court of Appeals has
determined that in a deprivation case, an attorney acting as both counsel for the child and guardian ad litem
is not a conflict of interest and an attorney can perform both roles with the permission of the court. Dawley
v. Butts Co. Dept. of Family and Children Services., 148 Ga. App. 815 (1979).
Another potential court participant is the Court Appointed Special Advocate, or CASA. CASA is an
organization operating in many counties within our state in which trained volunteers take an in-depth look
at an alleged case of deprivation and provide a report to the court at the adjudicatory and dispositional
hearings. Often the CASA and guardian ad litem work as a team, with the CASA having more time to do an
in-depth study of the family due to their relatively small caseload (they are usually limited to two cases at a
time). The CASA volunteer will, if possible, interview the child and his/her parents and make an oral or
written report of his/her observations to the court and any recommendation for disposition. CASA volunteers
are usually restricted to an advisory role for the court and do not call witnesses or present evidence.
However, if the CASA volunteer is also an attorney or if there is no attorney appointed to represent the
child, some courts will allow the volunteer to take a more active role in the proceedings.
[Typical Deprivation Graphic Goes Here.]
V. Filing of A Deprivation Petition](https://image.slidesharecdn.com/dfcsdocsimportant04112015-150714130648-lva1-app6891/85/Dfcs-docs-important-04112015-154-320.jpg)














![Page171 of 306
Georgia Compact Administrator will then notify DFCS of the decision of the receiving state. Regulation 7,
ICPC. The priority placement request and home study requires additional forms that can by obtained
through the Georgia Compact Administrator and are included at the end of this manual.
Under Article V of the ICPC, the sending state will retain jurisdiction over the child once an out of state
placement has been made. This jurisdiction continues until the child reaches the age of majority, becomes
self-supporting, is adopted, or until the child case is cleared with the concurrence of the compact
administrator in the receiving. This means that the juvenile court will retain jurisdiction over all decisions in
regard to custody, supervision, care, treatment and disposition of the child. The sending state will also
continue to have financial responsibility for the child just as it would in an in-state placement.
[Insert Citizen Review Graphic Here.]
VIII. Permanency Planning - Judicial and Citizen
Review
A. 30-Day Case Plans
An order of disposition placing a deprived child in foster care under the supervision of the Division of Family
and Children Services is in effect for up to 12 months after the original placement unless it is terminated
sooner by the court. O.C.G.A. § 15-11-58(k). All other dispositional orders will remain in force for two years
unless sooner terminated by the court. O.C.G.A. § 15-11-58.1(a). Within 30 days of the date of the removal
of the child where the child has not already been returned to his/her parent(s), DFCS must submit a written
report to the court which shall either include a case plan for the reunification of the family or the ba sis for its
determination that a plan for reunification is not appropriate. O.C.G.A. § 15-11-58(b).
The contents of the report shall be based upon a meeting to be held between DFCS and the parents and
children in question. This meeting should be held in consultation with the Citizen Review Panel if one exists
in your county. The parents shall be given written notice of the meeting at least five days in adva nce and
shall be advised that the report to be discussed at this meeting will be submitted to the judge to become an
order of the court. O.C.G.A. § 15-11-58(b). You should be aware that if the dispositional hearing occurs
within 30 days of the removal of the child, the juvenile court judge in your jurisdiction may ask you to
provide this report to the court sooner than required by law. Regardless of where in the court process the
case is, DFCS must submit a written report to the court within 30 days of the removal of the child. If a 30-
day case plan is submitted to the court which contains a plan for reunification services, it must address each
of the following items:
1. Each reason requiring the removal of the child;](https://image.slidesharecdn.com/dfcsdocsimportant04112015-150714130648-lva1-app6891/85/Dfcs-docs-important-04112015-171-320.jpg)




![Page176 of 306
(1982). A dispositional order which is allowed to expire before a proper extension is given by the juvenile
court would seem to require the return of the child to his parent(s) or guardian. However, nothing at this
point would permit DFCS from filing a new deprivation petition requesting that the child be removed from
the home once again. The Court of Appeals has previously refused to overturn a judgement of the trial court
temporarily extending custody with DFCS on the last day before a dispositional order was set to expire until
another deprivation petition could be filed. In the Interest of P.M., et al., children., 201 Ga. App. 100
(1991). In that case, the court held an emergency hearing to extend custody without providing notice to the
child's mother. By the time the case reached the Court of Appeals, the trial court had held an adjudicatory
hearing on the merits of the new deprivation petition and had once again ordered the child removed from
the home. The court declined to reverse an improper extension order because the trial court had found once
again by clear and convincing evidence that the child was deprived and therefore the issue was not
reviewable because of the new adjudicatory hearing. Id. at 100. It would seem that a juvenile court judge
could issue an emergency (shelter care) order if the child is in danger and the prior order granting DFCS
temporary custody expires without an extension. However, in order to prevent unnecessary trauma to the
child as well as having to start the deprivation proceeding all over again, it is important for the case
manager to coordinate with the SAAG to ensure that motions to extend custody are filed with in plenty of
time to allow for a hearing prior to the expiration of the original order.
The repeated use of motions to extend temporary custody without attempting to terminate parental rights
has caused some to criticize this practice as promoting "foster care drift". This is the movement of a child
from one temporary foster home to another while waiting (sometimes in vain) for the parent(s) to comply
with the court ordered reunification plan. Some observers have questioned whether motions to terminate
should be pursued sooner in order to provide the child with a more permanent arrangement. In a survey of
DFCS case managers conducted by the Child Placement Project, over forty percent (40%) of the
respondents reported that motions to extend temporary custody were filed in more than half of all
deprivation cases.
[Insert 30-day Graphic Here.]
IX. Termination of Parental Rights
A petition for the termination of parental rights is often made by the Division of Family and Children
Services when it appears that efforts to reunify the family will either be futile, or will potentially harm the
child. A termination petition can also be filed on behalf of the child by any other party who knows the facts
contained in the petition and believes that they are true just as with a deprivation petition. O.C.G.A. § 15-
11-95(b). An order terminating parental rights has the effect of ending all rights and obligations of the
parent with respect to the child and/or the child to the parent, including the right of inheritance. The parent
will have no right to notice of or the right to object to the future adoption of that child into another
home. O.C.G.A. § 15-11-93. The termination of one parent's rights with respect to the child has no effect on
the rights of another legal parent to the care and control of that child. O.C.G.A. § 15-11-105.
A. Standard of Proof and Requirements for Termination](https://image.slidesharecdn.com/dfcsdocsimportant04112015-150714130648-lva1-app6891/85/Dfcs-docs-important-04112015-176-320.jpg)







![Page184 of 306
the child to another placement. O.C.G.A. § 15-11-103(d).
In order for a termination of parental rights to move smoothly, it is important for the DFCS case manager to
identify blood relatives and the putative father of the child as soon as possible after the child comes into
temporary custody with the department. This will prevent unnecessary delays once the termination petition
is filed as well as preventing the placement of a child with another "stranger" after a long period in foster
care simply because that person is related to the child by birth.
[Insert 2-Step TPR Test Here.]
X. Evidence
When testifying in court, case managers will often witness evidentiary arguments between la wyers for which
they have not been prepared. This chapter is an effort to give you a very basic understanding of evidence
law as applied in juvenile court. The manual covers only the topics which we feel you may encounter during
your career and is not an authoritative review of Georgia evidence law. We hope that you will find it useful
in understanding what information is admissible in court.
There are three main types of evidence. Testimonial Evidence basically involves an attorney (such as a
SAAG) calling a witness (such as a DFCS case manager) to the stand to ask him/her questions. This is called
direct examination. The opposing attorney (usually representing the parents), will have an opportunity to
cross examine the witness. Documentary Evidence basically covers written materials such as case reports,
letters, memos, hospital and school records, etc. Demonstrative Evidence includes what you would consider
"pieces of evidence" such as objects, photographs, etc, as well as charts, graphs, and other visual aides.
One important restriction on evidence is that it must be "relevant." The Georgia Court of Appeals has held
that evidence is relevant if it logically tends to prove or disprove any material fact which is at issue in the
case. Kelly v. Floor Bazaar, Inc., 153 Ga. App. 163,165 (1980). In addition, if evidence has any tendency to
advance a party's position at trial, it is relevant. It is for the fact finder (the judge) to decide how credible
this evidence is. Daniels v. State, 184 Ga. App. 689 (1987). As you can probably see, it is fairly easy to find
some justification to call a piece of evidence relevant and most objections on this basis fail for that reason.
In the area of testimonial evidence, competence is another restriction that must be dealt with when calling
child witnesses to the stand. In deprivation hearings, the child on whose behalf the petition is filed can in
some situations be a key witness. O.C.G.A. § 24-9-5(a) provides that children who do not understand the
oath (to tell the truth, the whole truth, and nothing but the truth) shall be incompetent witnesses who will
not be allowed to testify. However, if a child witness is the subject of a deprivation hearing, such a child is
automatically competent to testify by law. O.C.G.A. § 24-9-5(b). If other children are called to the stand](https://image.slidesharecdn.com/dfcsdocsimportant04112015-150714130648-lva1-app6891/85/Dfcs-docs-important-04112015-184-320.jpg)