Developmental trajectory from newborn to infancy 1.pptx
1.
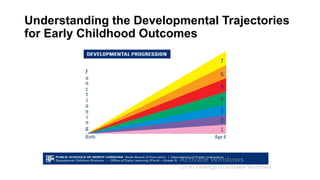
DEVELOPMENTAL TRAJECTORY
FROM NEWBORNTO INFANCY
Normal and abnormal
Presenter : Dr Neelam
Moderators: Dr Nisha K Bhatta
Dr Shyam Prasad Kafle
Dr Lokraj Shah
Dr Ranjana Bista
2.
Outlines
• Development trajectory
•Understanding the developmental trajectories
• Variations in general pattern of development
• Normal development
• Factors affecting development
• Science of early childhood development
• Developmental theories
• Abnormal development
3.
Developmental trajectories
• Developmentallines or sequences of changes leading up to particular attainments in
a particular developmental domain.
• Complex skills laid down on a foundation of simpler ones
• 1st year of life set the trajectory for a child's life.
Variations in theGeneral Pattern of Development
1. Average.
2. Average, becoming advanced.
3. Advanced in certain fields.
4. Advanced in all fields.
5. Average or advanced, deteriorating, or slowing down in development.
6. Delayed in all fields.
7. Delayed in all fields, becoming average or advanced.
8. Delayed in some fields.
11.
Normal Development
A completelydependent baby gradually transitions into an ambulatory child who can express
thoughts and look after himself.
Through five developmental stages:
• Cognitive development
• Social or emotional development
• Speech and language development
• Fine motor development
• Gross motor development
12.
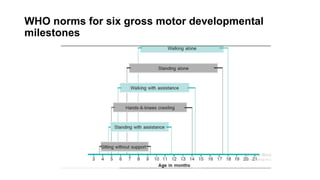
WHO norms forsix gross motor developmental
milestones
The interactive influencesof genes and
experience shape the developing brain.
• “Serve and return” relationship between children and their parents
• Young children naturally reach out for interaction:
• Vocalizations
• Facial expressions
• Gestures
• Adults respond to children
• In the absence of such responses disparities in learning and behavior.
18.
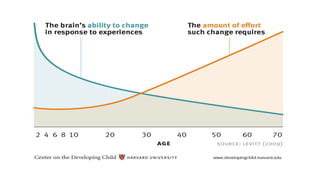
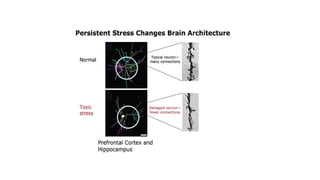
Brain’s capacity forchange decreases with age
• Maturing brain becomes more specialized
-Less capable of reorganizing
• “Windows” for language learning and other skills remain open
- Increasingly difficult to alter over time.
20.
Toxic stress damagesdeveloping brain
architecture
• Unrelenting stress in early childhood toxic to the developing brain.
• Absent support toxic stress becomes built into the body
22.
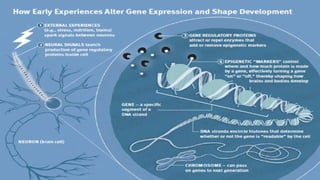
Epigenetics and childdevelopment
• Environmental influences—children’s experiences
-Affect the expression of their genes.
• Old idea that genes are “set in stone” has been disproven.
• Nature vs. Nurture is no longer a debate. It’s nearly always both!
24.
Young brains areparticularly sensitive to epigenetic
changes
• Epigenetic adaptations –
Influence when, and how genes release their instructions for building
• Future capacity for health, skills, and resilience.
• Supportive and nurturing experiences in the earliest years-
• Generate positive epigenetic signatures
• Activate genetic potential
Psychoanalytic theory
• Sigmundfrued
• Explain importance of early experiences on development
• Frued’s psychosexual stages of development:
Oral stage Birth to 1y
Anal stage 1 to 3y
Phallic stage 3 to 6y
Latent stage 6 to 11y
Genital stage 11 to 18y
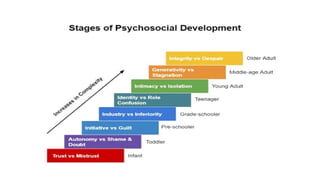
Psychosocial theory
• EricErikson
• Expanded on Frued’s theories
• Believed that
• Development occurs life long
• Acquires attitudes and skills
• Successful negotiation of the psychological conflict.
30.
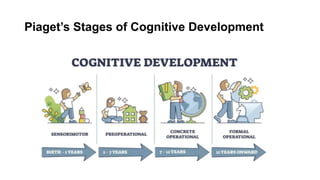
Cognitive development theory
•Jean Piaget
• Construct understanding of the world through active involvement and interactions
• Children’s understanding as their “schemas”
• Used as
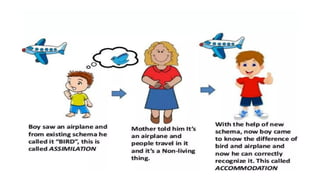
• Assimilation
• Accommodation
Socio-cultural theory
• LevVygotsky
• Active learners
• Knowledge is socially constructed.
• Cultural values and customs dictate
• Important to learn
• Learn from more expert members of the society
34.
Abnormal development
• Developmentdoesn’t follow the normal course
• Unusual pattern of behavior, emotion or thought.
• Can occur at any stage of development.
• Initial few days after birth is most vulnerable
• Caused by early traumatic experiences or toxic stress
Causes of abnormal/atypicaldevelopment
Fine motor delay
• Intellectual disability
• Blindness
• Severe hypo or hypertonia (cerebral palsy)
38.
Causes of abnormal/atypicaldevelopment
Social or emotional delay
• Intellectual compromise
• Blindness
• Autism
• Mobius syndrome
• Myotonic dystrophy
39.
Causes of abnormal/atypicaldevelopment
Delayed speech or language
• Preterm or small for dates
• Hydrocephalus
• Tuberculous or other pyogenic meningitis
• Intellectual disability
40.
Causes of abnormal/atypicaldevelopment
• Hearing defects
• Developmental expressive or receptive aphasia
• Cerebral palsy
• Psychogenic cause
41.
Causes of abnormal/atypicaldevelopment
Cognitive delay
• Low intelligence
• Emotional factors
• Environmental factors
• Delayed maturation
• Poor teaching
• Visual, auditory and spatial difficulties
• Genetic factors (‘specific dyslexia’) or specific learning disorders
42.
Alarm bells foran atypical development
• Delays in achieving milestones
• Atypical movement patterns- repetitive and or excessive movements
• Difficulty in following simple instruction and learning new skills
• Limited use of words or gestures to communicate needs
• Lacking reciprocity in play, social, or sensory routines
• Poor eye-contact/smiling
• No pretend or imaginary play
43.
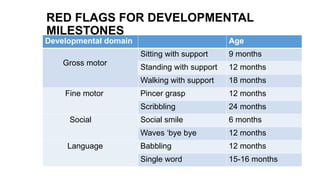
RED FLAGS FORDEVELOPMENTAL
MILESTONES
Developmental domain Age
Gross motor
Sitting with support 9 months
Standing with support 12 months
Walking with support 18 months
Fine motor Pincer grasp 12 months
Scribbling 24 months
Social Social smile 6 months
Waves ‘bye bye 12 months
Language Babbling 12 months
Single word 15-16 months
44.
Developmental surveillance vsdevelopmental
screening
Developmental surveillance:
- Documenting developmental history
- Eliciting parental concern
- Developmental examination
• Developmental screening
-Standardized tests to identify children
who require further diagnostic
assessment
- To identify risk of developmental
disorders
- Norm- referenced tests are used
45.
DEVELOPMENTAL SCREENING TEST`
Questionnaire based
• Parents’ evaluation of
developmental status (PEDS)
• Ages and Stages Questionnaire
• Developmental profile II/III
• ICMR Psychosocial development
screening test
Examination based
• Denver developmental screening
test II (now out of date)
• Bayley Infant neurodevelopment
screen (BINS)
• Phatak’s Baroda Screening test
• Trivandrum Development Screening
test
• Amiel-Tison test
46.
When to do?
Developmental screening using a formal, validated, and standardized scale
• During the 1st 3 yr of life at 9 m, 18 mo, and 30 mo.
High risk infants :
• 4-6 months
• 9-12 months,
• 18-24 months
• Yearly till 5 years of age
• Once at school entry.
Autism screening test at the 18 and 24 mo visits.
47.
Take home message
•All children are different. They differ in the rate of development as a whole, and in the rate and
pattern of development within each field, leading to variations in developmental trajectories.
• There is no dividing line between normal and abnormal, the further away from the average he is, the
more likely he is to be abnormal.
• Various factors affect the developmental trajectory. This is governed by different theories of
development.
• First year of life provides a new challenge, it is possible to identify developmental anomalies in this
window of time via early developmental screening.
• Early intervention help children achieve near normal potential.
#3 The concept of developmental trajectories recognizes that complex skills build on simpler ones. prenatal period and the 1st yr of life provide the platform for remarkable growth and development
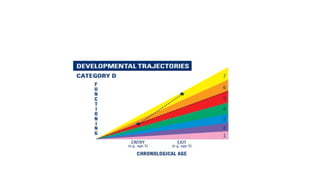
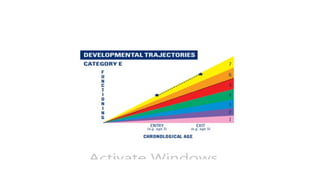
#4 1-Not yet age expected, 2-between nearly and not yet, 3-nearly age expected, 4- between somewhat and nearly, 5-somewhatage expected, 6-between completely and somewhat, 7-completely age expected. Based on this, children’s dev trajectories are divided into five categories:
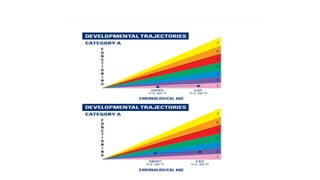
#5 Category A: children who did not improve functioning-Children who acquired no new skills or regressed during their time in the program, Didn’t gain or use even one new skill, Children with degenerative conditions/significant disabilities, Rated lower at exit than entry; OR Rated 1 at both entry and exit;
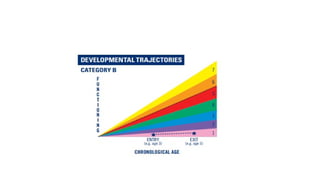
#6 Progress category B:Children who improved functioning but not sufficient to move nearer to functioning comparable to same-aged peers -Acquired new skills but continued to grow at the same rate throughout their time in the program, Gained and used new skills but did not increase their rate of growth or change their growth trajectories,Rated 5 or lower at entry (below age level); AND Rated the same or lower at exit
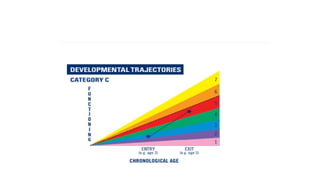
#7 PROGRESS CATEGORY C: Children who improved functioning to a level nearer to same-aged peers but did not reach age level expectations-Acquired new skills and accelerated their rate of growth during their time in the program, Made progress toward catching up with same-aged peers but were still functioning below age expectation when they left the program, Changed their growth trajectories & “narrowed the gap”, Rated higher at exit than entry; AND Rated 5 or below at exit(below age level)
#8 PROGRESS CATEGORY D: Children who improved functioning to reach a level comparable to same-aged peers-Children who were functioning below age expectation when they entered the program but were functioning at age expectation when they left, Started out below age expectation, but caught up, Rated 5 or lower at entry (below age level); AND Rated 6 or 7 at exit
#9 PROGRESS CATEGORY E: Children who maintained functioning at a level comparable to same-aged peers- Children who were functioning at age expectation when they entered the program and were functioning at age expectation when they left, Rated 6 or 7 at entry; AND, Rated 6 or 7 at exit
#10 many variations from the usual pattern of development that cause difficulties in developmental diagnosis. The truly average child, the child who is average in everything, is a rarity. Some appear to be merely average at first, but later prove to be intellectually superior; it may be that the early developmental tests failed to detect the signs of superiority, or else full maturation was delayed. Advanced or delayed in certain fields of development-because of a familial trait, disability. slows down- Down’s syndrome, deterioration-emotional deprivation, poor education, degenerative ,diseases, psychosis, encephalitis or metabolic diseases, Delay in all fields-intellectual disability, delayed maturation
#11 Child acquires varoius skills for optimal functioning in orderly fashion through five developmental stages during predictable timeperiods or age stages. Development through these stages run parallel to the maturational changes occurring in the brain.
#12 expected to be attained within a certain age range.
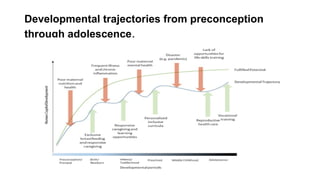
#15 These risk fac and protective factors interact to determine the dev trajectory from preconception through adolescence. In presence of protective fac children attain their dev potential. Prescence of variety of risk fac in early life lowers the dev trajectory of the child.
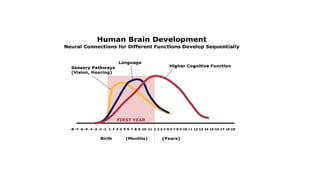
#16 Ongoing process, from before birth into adulthood.Initial few days after birth is most vulnerable. Neuronal plasticity, critical to learning and remembering (and therefore development) is at its peak during this time, which permits neuronal networks in CNS to reorganize in response to environmental stimulation, both positive and negative. Periods of rapid development generally correlate with periods of great changes in synaptic numbers in relevant areas of the brain. After first few years of life, brain circuits become more specialized and efficient.
1 – Sensory pathways like for basic vision and hearing
2 - Language skills
3 - Higher cognitive functions
#17 Serve and return works like a game of tennis or volleyball between child and caregiver. The child “serves” by reaching out for interaction—with eye contact, facial expressions, gestures, babbling, or touch. A responsive caregiver will “return the serve” by speaking back, playing peekaboo, or sharing a toy or a laugh. if the responses are unreliable or inappropriate—the brain’s architecture does not form as expected,
#18 As brain is most flexible, or plastic, early in life to accommodate a wide range of environments and interactions, it is easier and more effective to influence a baby’s developing brain architecture. As the maturing brain becomes more specialized to assume more complex functions, it is less capable of reorganizing and adapting to new or unexpected challenges.
#22 How children experiences affect their genes and it is very impt concept to know as epigenetics has lifelong impact on dev trajectories. The brain is particularly responsive to experiences and environments during early development.
#23 These gene regulatory proteins head to the nucleus of the neural cell, where they either attract or repel enzymes that can attach them to the genes.
Our genes provide the blueprint, but the early environments in which children live leave a lasting signature on those genes. the very best strategy is to support responsive relationships and reduce stress to build strong brains from the beginning.
#24 Experiences very early in life, when the brain is developing most rapidly, cause epigenetic adaptations. That’s why it’s crucial to provide supportive and nurturing experiences for young children in the earliest years.
#26 An infant’s primary interaction with the world is through the mouth. The mouth is vital for eating, and the infant derives pleasure from oral stimulation through gratifying activities such as tasting and sucking. If this need is not met, the child may develop an oral fixation later in life, eg of which include thumb-sucking, smoking, fingernail biting, and overeating.
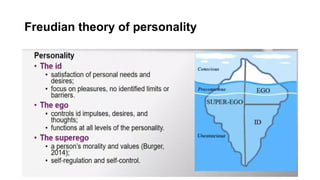
#27 Frued compared the mind to an iceberg. Concious mind- tip of iceberg, these are the thoughts we are aware of. Submerged part of iceberg is the unconscious mind-desires and memories that we don’t actively think about.
#28 Believed that each stage of dev was focused on overcoming a conflict. Success or failure in dealing with these conflicts at each stage can impact overall functioning of a person. He proposed a theory that had 8 stages and in each stage people face new challenges and outcome depends on how people handle these challenges.
#29 infant will develop a healthy balance between trust and mistrust if cared for and responded to consistently. Abuse or neglect will foster mistrust. Positive outcomes consist of the development of hope and drive. Toilet training is a significant part of this stage. Positive outcomes consist of willpower and self-control, while negative outcomes could contribute to compulsive behaviours. Initiative means self-confidence to perform actions, even with understanding of risks and failure. Guilt results from believing an action will draw disapproval. Positive outcomes foster purpose and direction, while negative outcomes encourage inhibition. Industry means having meaningful activity and the competence to perform a skill. Inferiority means feeling incapable of experiencing failure or inability to discover one’s own strengths.Positive outcomes foster competence, while negative outcomes encourage inertia.
#30 Piaget described how children actively construct knowledge for themselves through the linked processes of assimilation (taking
in new experiences according to existing schemata) and accommodation(creating new patterns of understanding to adapt to new information)
#32 Piaget divided child development into 4 stages. Sensorimototr is the time when children master 2 phenomena- causality and object permanence. Infants use their sense and motor abilities to manipulate their surroundings and learn abt the envt. They understand cause and effect relationship, like how crying can make parents rush to give them attention. This is emergence of thought and allows for the planning of actions.preoperational-when child can use mental representations such as symbolic thought and language. Children learn to imitate and pretend play. This stage characterized by egocentrism.3rd stage-child uses logical operations when solving problems4th stage-suggest adolescent can use logical operations with the ability to use abstractions.
#33 Lev believed tht children actively through hands on experience and their knowledge are socially constructed. Parents, caregivers, cultural beliefs, values, and language are all responsible for dev of this higher order function of learning. He said child internalizes information they get from interaction with others. So he was all about how we as individual are influenced by those around us and culture around us. This theory stresses the importance of social interaction in dev of cognition.
#35 Delay-development occur in its usual sequence but at a slower rate, with milestones achieved later than the normal range.Developmental dissociation indicates delay in a single stream with typical development in other streams, e.g. Autism. Deviancy or deviation is defined by development occurring out of sequence, as when a child stands before sitting (as in diplegic cerebral palsy) or has better expressive vocabulary than receptive understanding of words (language and autism spectrum disorders). Regression refers to a loss of skills, e.g. Rett syndrome
#36 Temperament describes the stable, early-appearing individual variations in behavioral dimensions, including emotionality (crying, laughing, sulking),
activity level, attention, sociability, and persistence. These characteristics lead to 3 common constellations: (1) the easy, highly adaptable child, who has regular biologic cycles; (2) the difficult child, who is inflexible, moody, and easily frustrated; and (3) the slow-to-warm-up child, who needs extra time to adapt to new circumstances. Temperament has long been described as biologic or “inherited.” Monozygotic twins are rated by their parents as temperamentally similar more often than are dizygotic twins. The concept of temperament can help parents understand and accept the characteristics of their children.