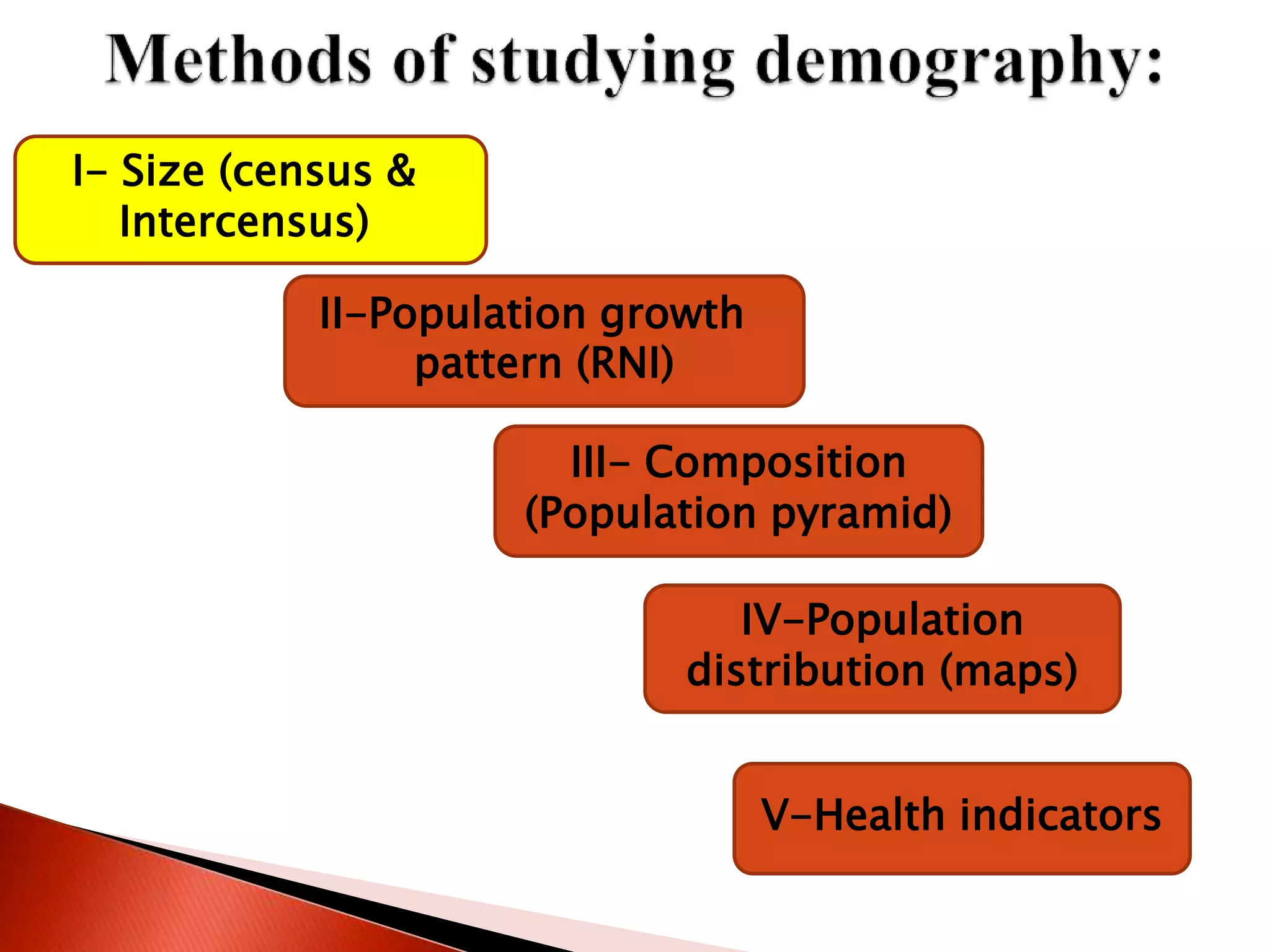
This document defines key concepts in demography and describes methods for studying population characteristics and changes over time. It discusses population estimation methods including census data collection and calculating intercensus population sizes. It also describes population pyramids and their characteristics for analyzing population composition. Finally, it defines different types of vital rates and health indicators used to describe and compare community health.

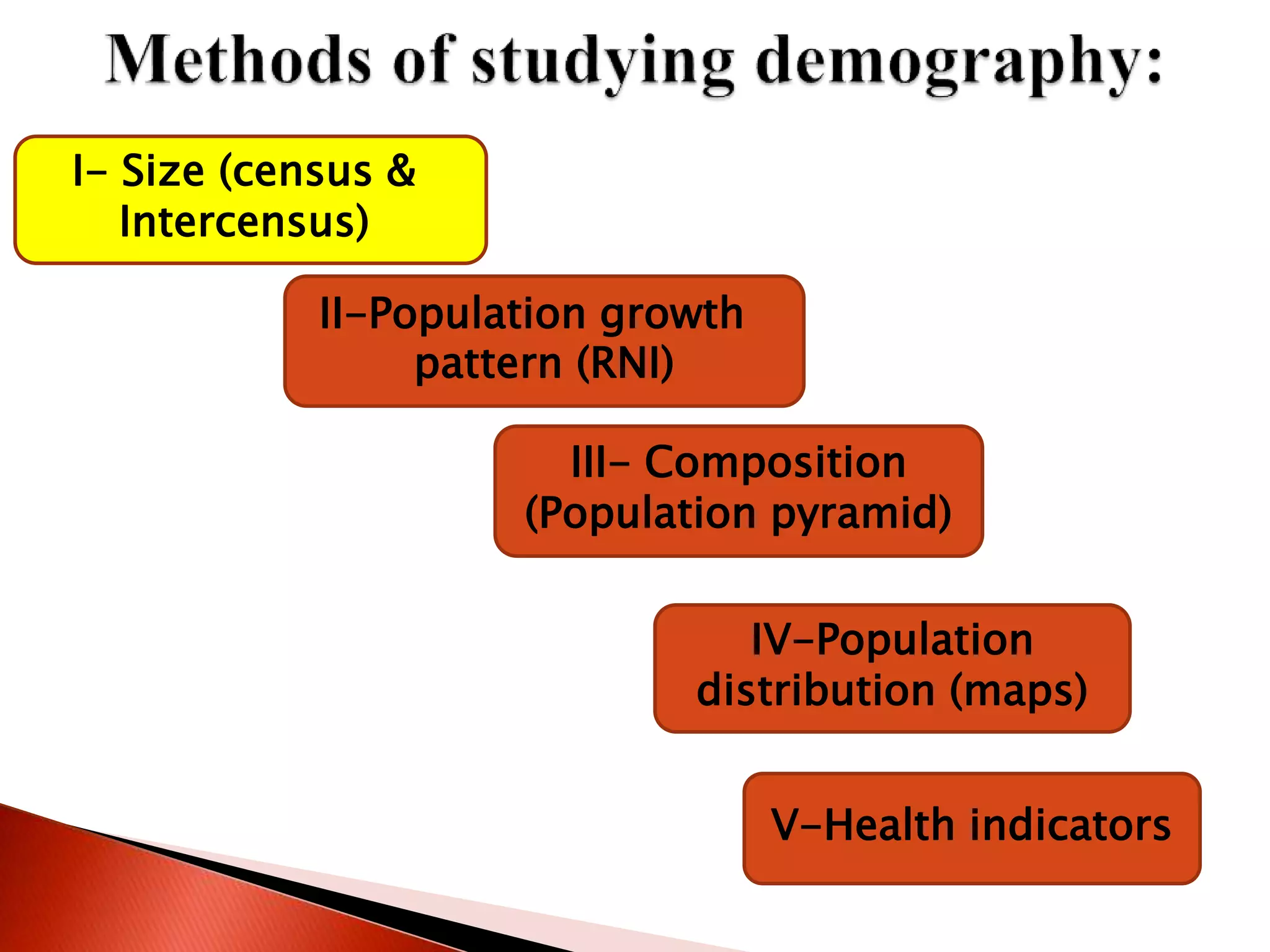
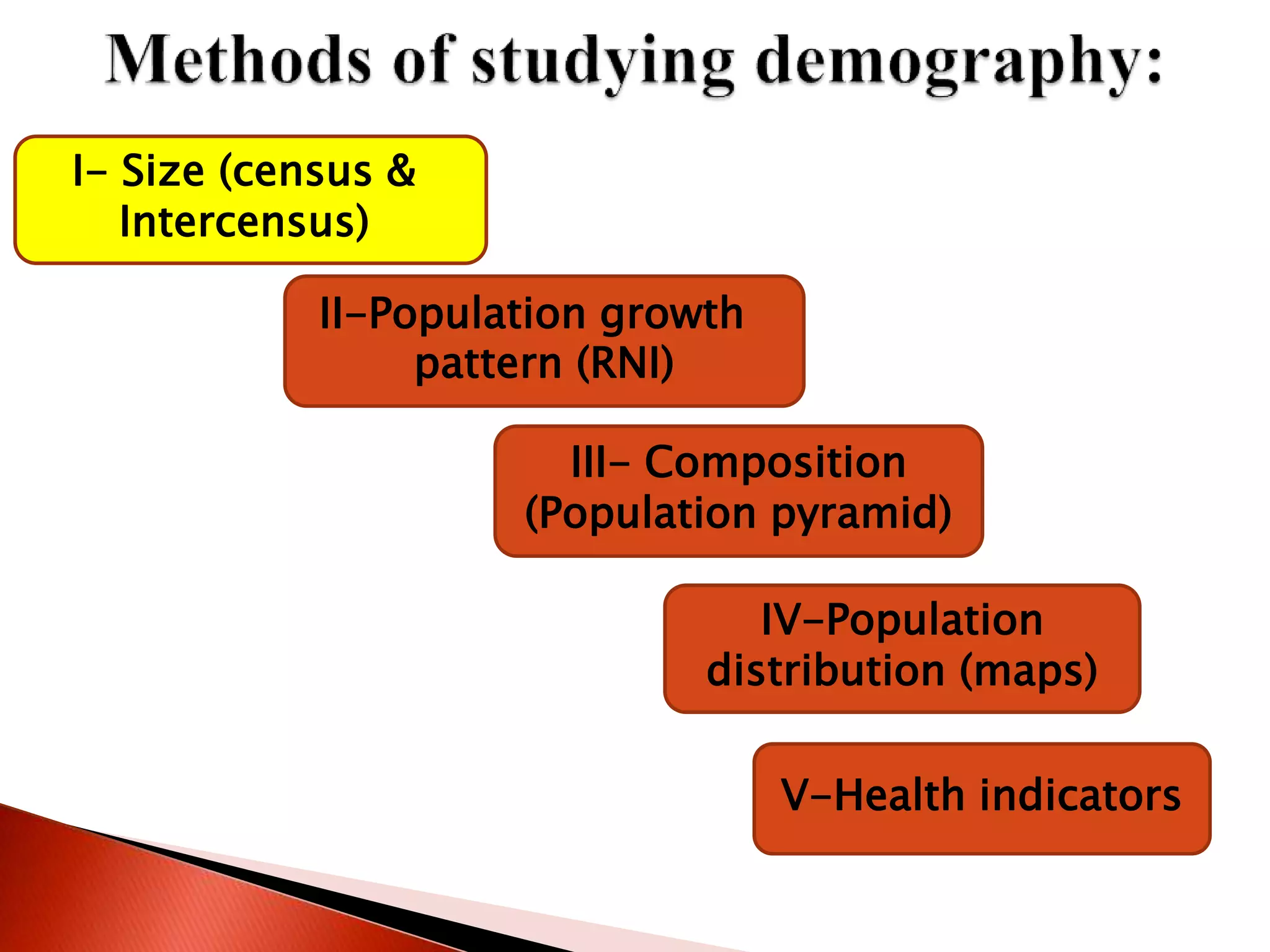
![ Define demography and recognize its importance
and methods of study.
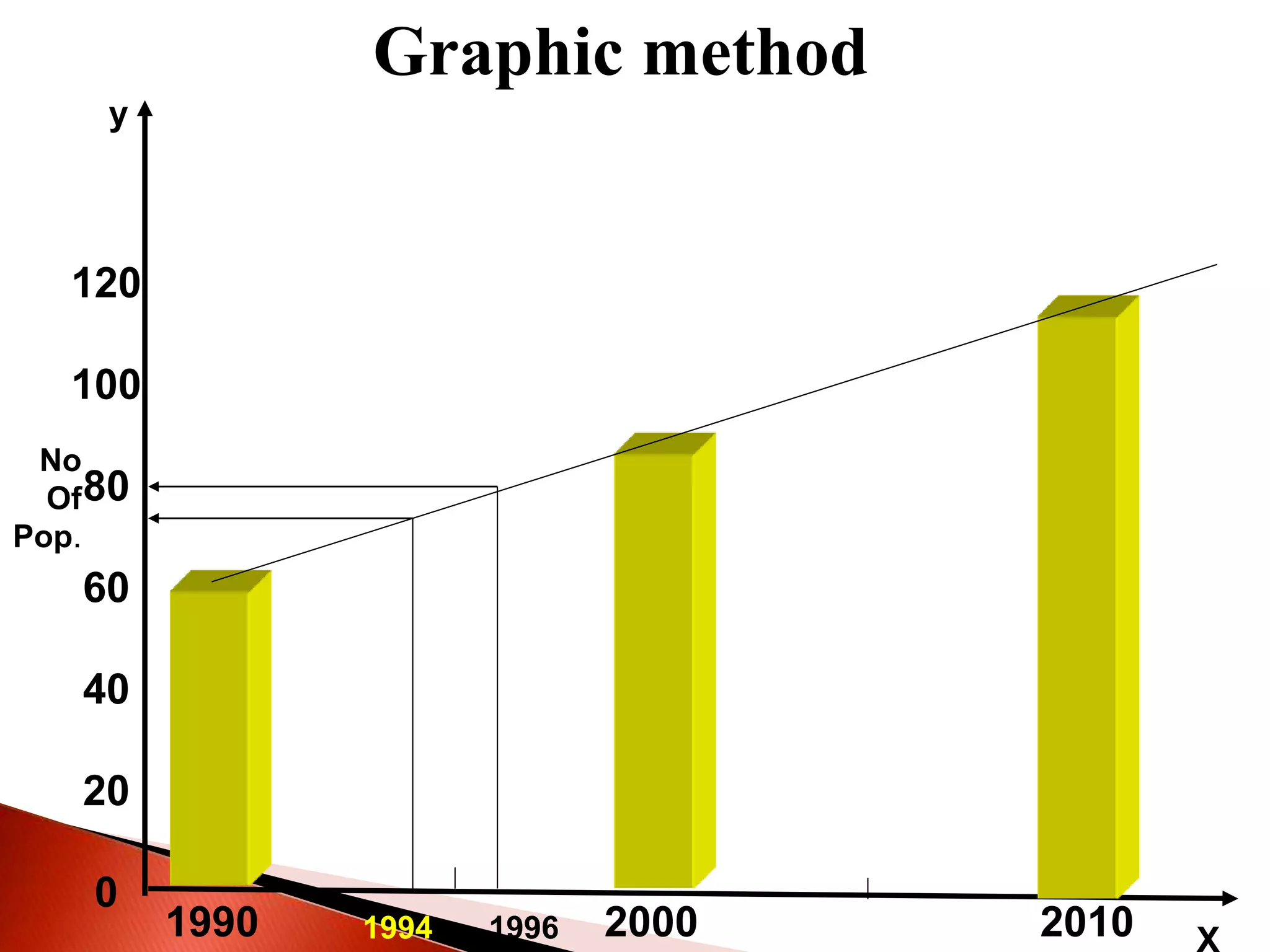
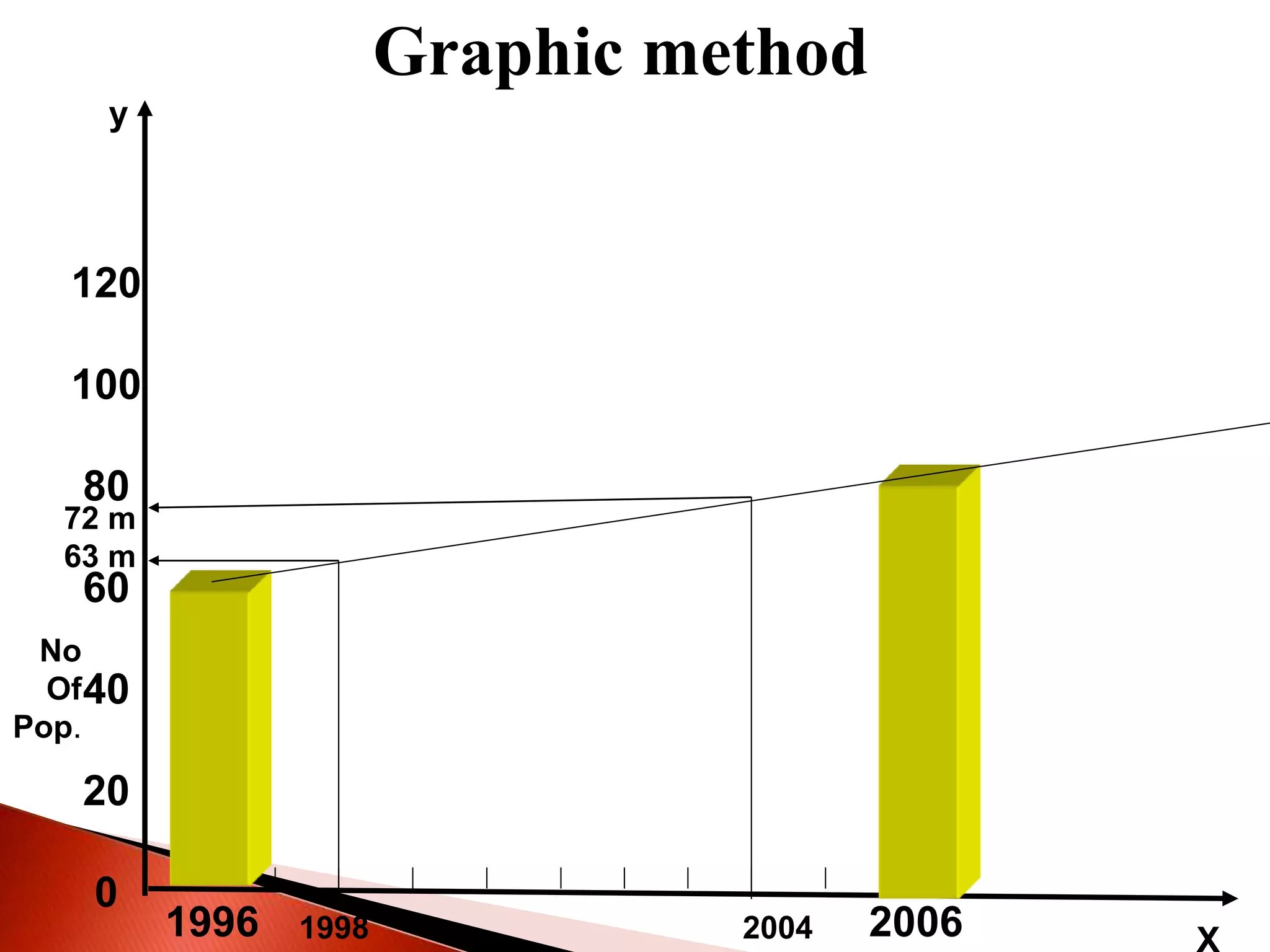
Describe population estimations in the census and
inter-census years.
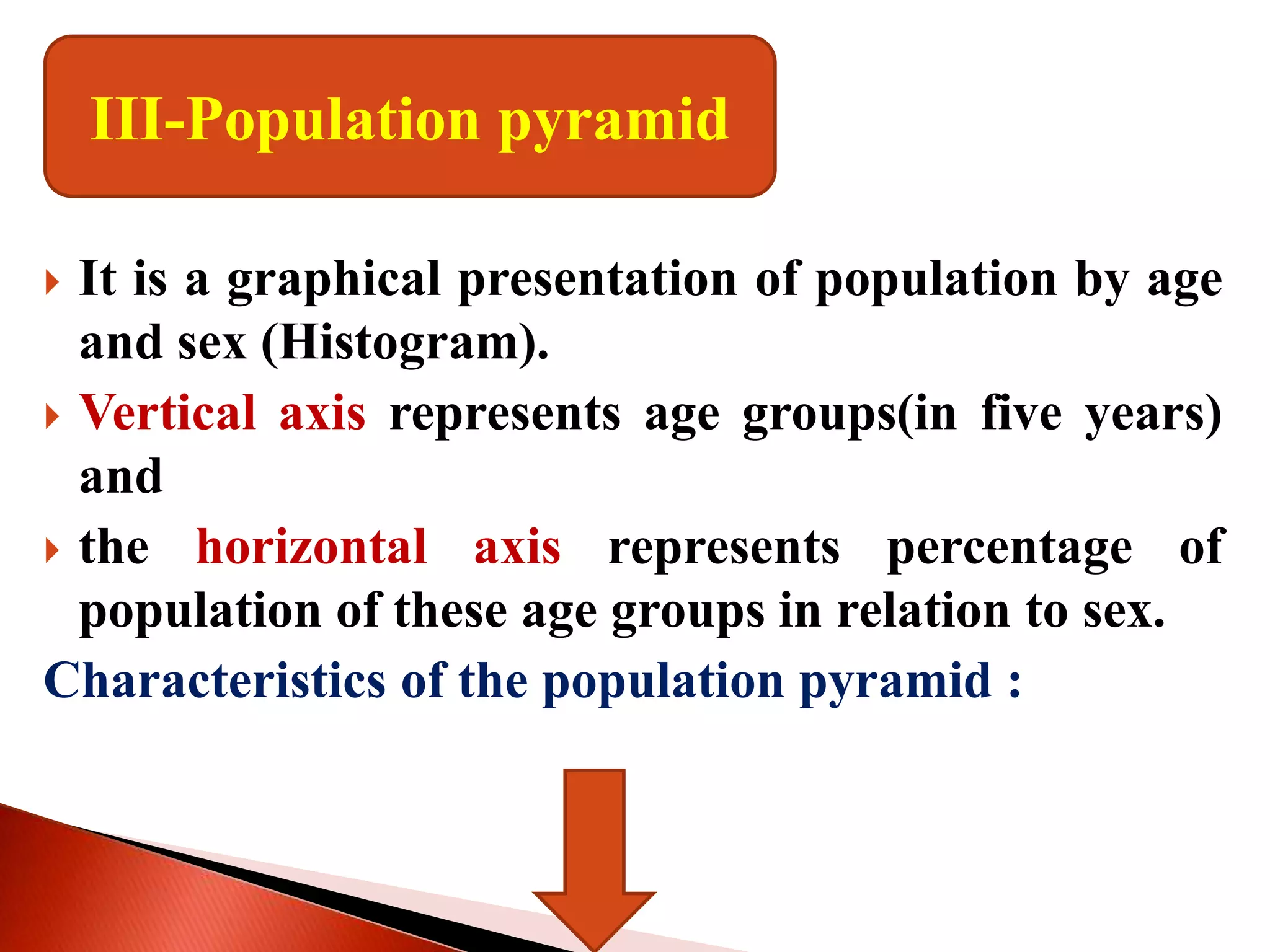
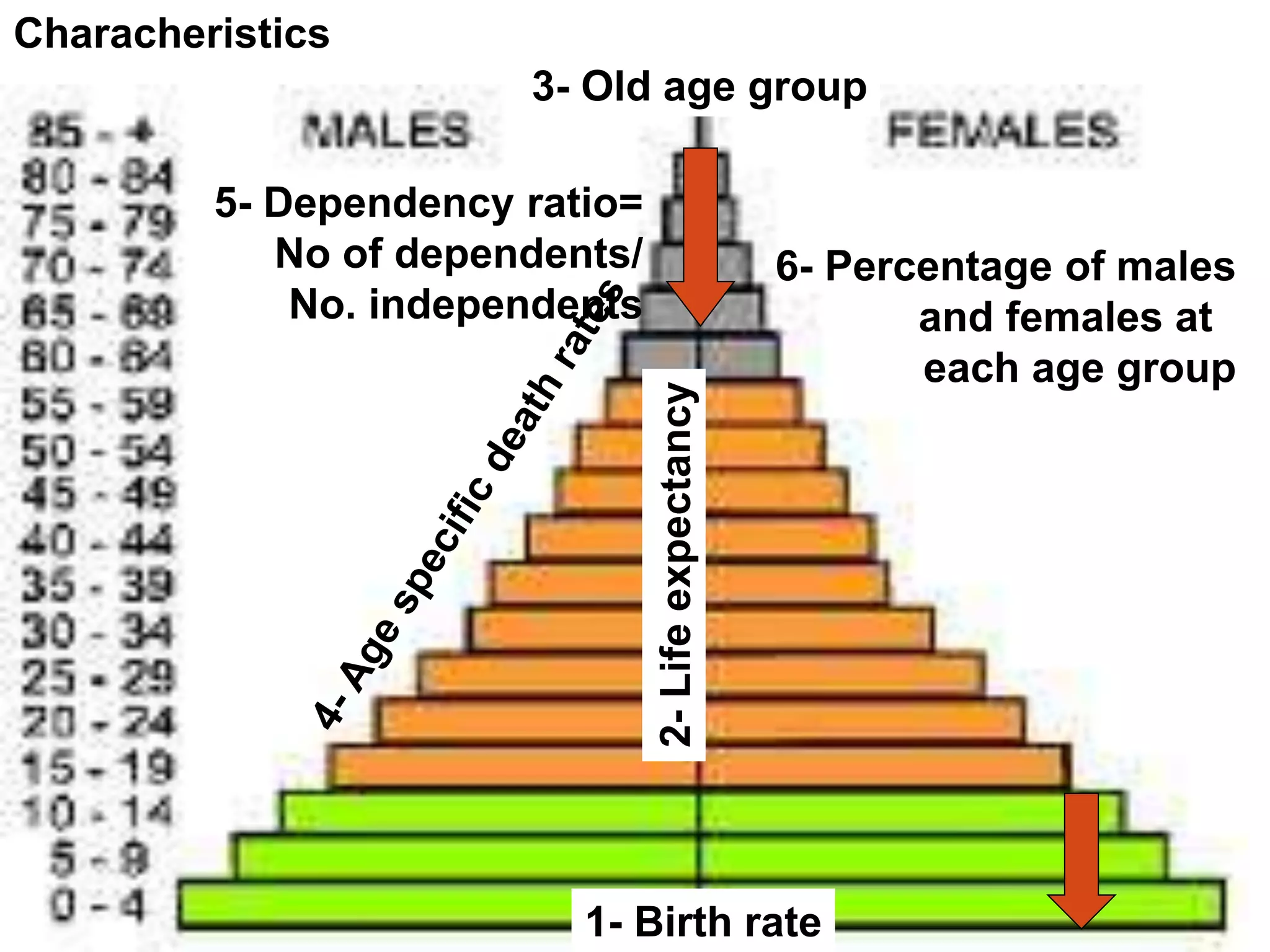
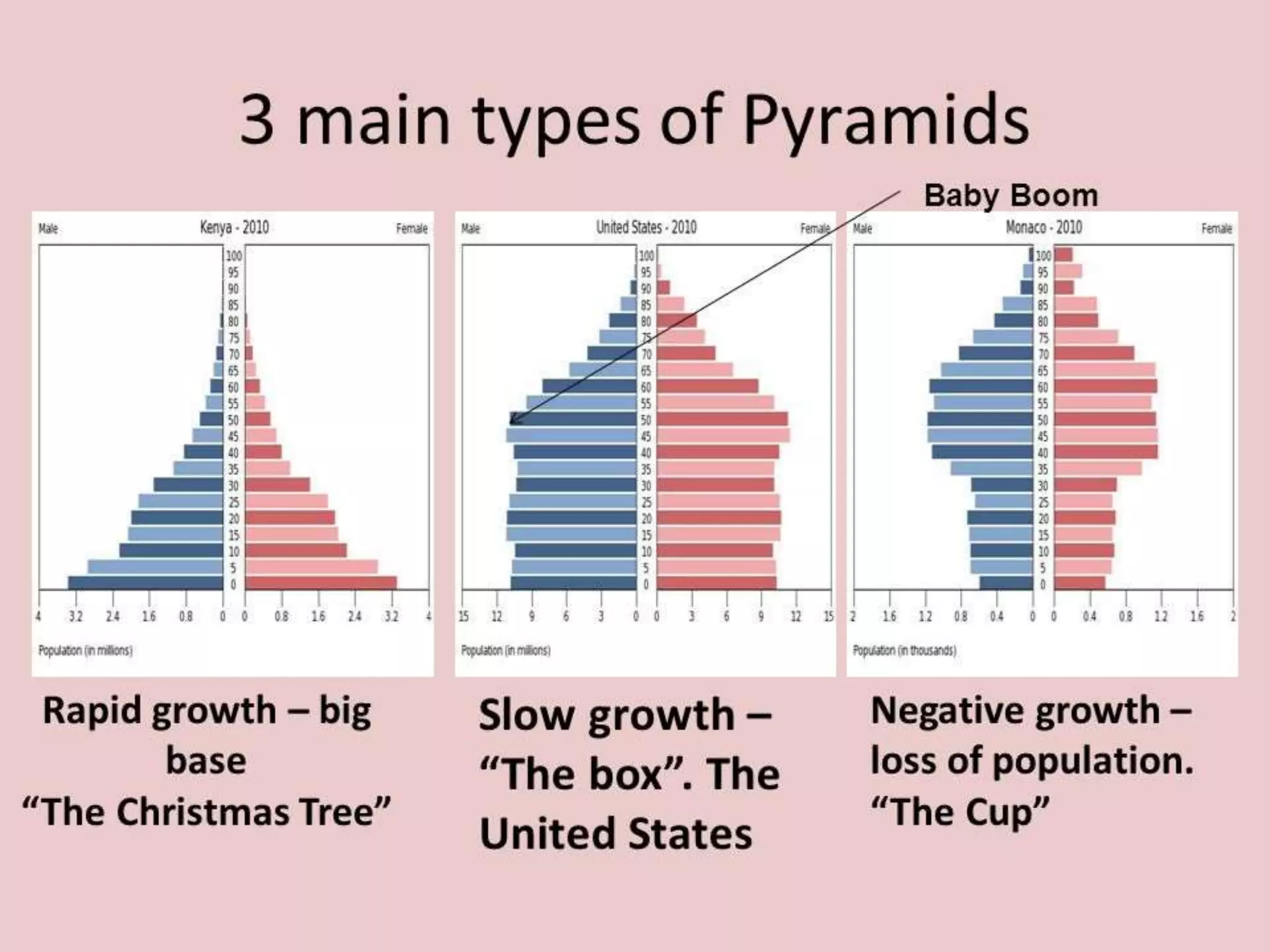
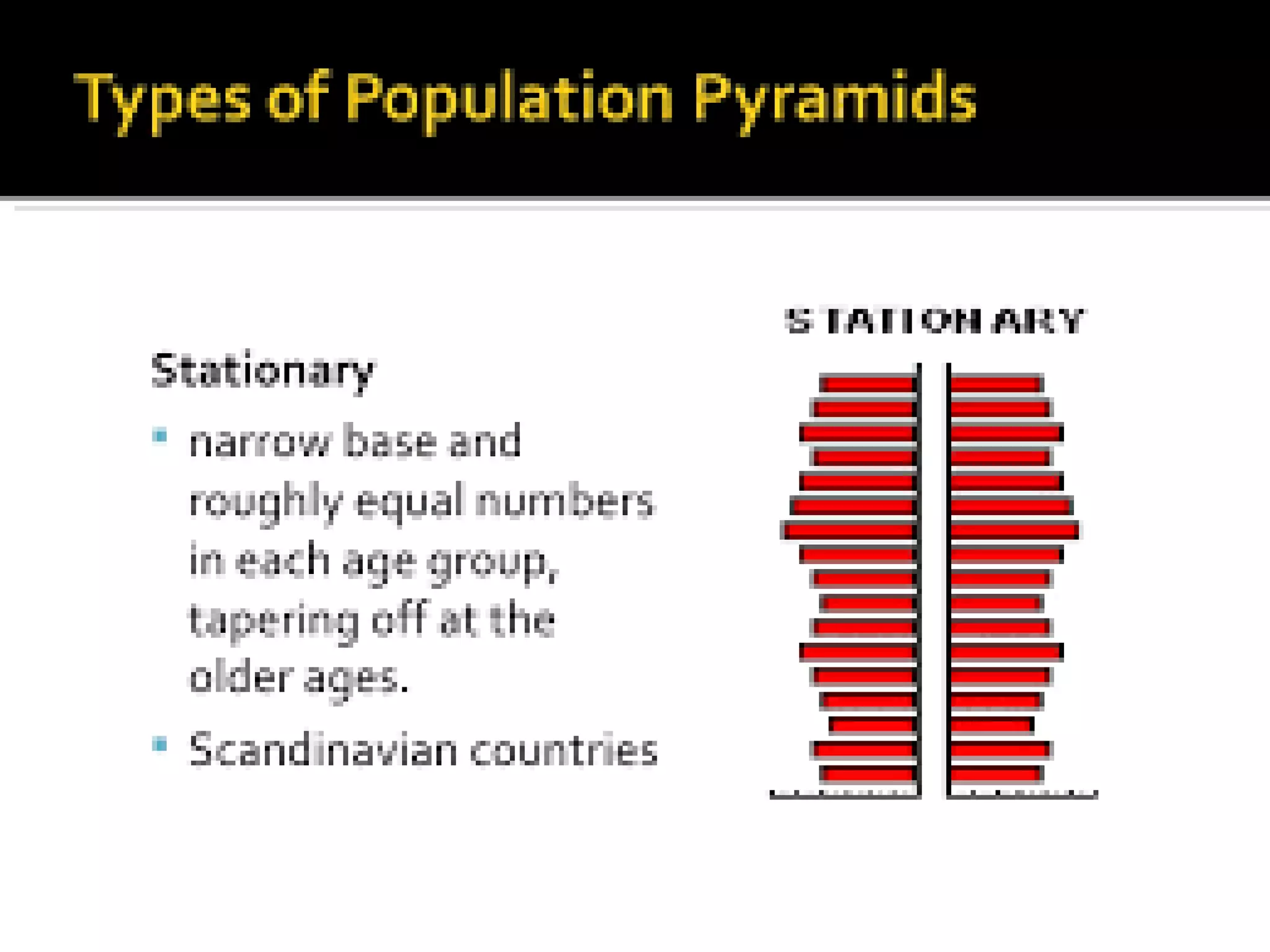
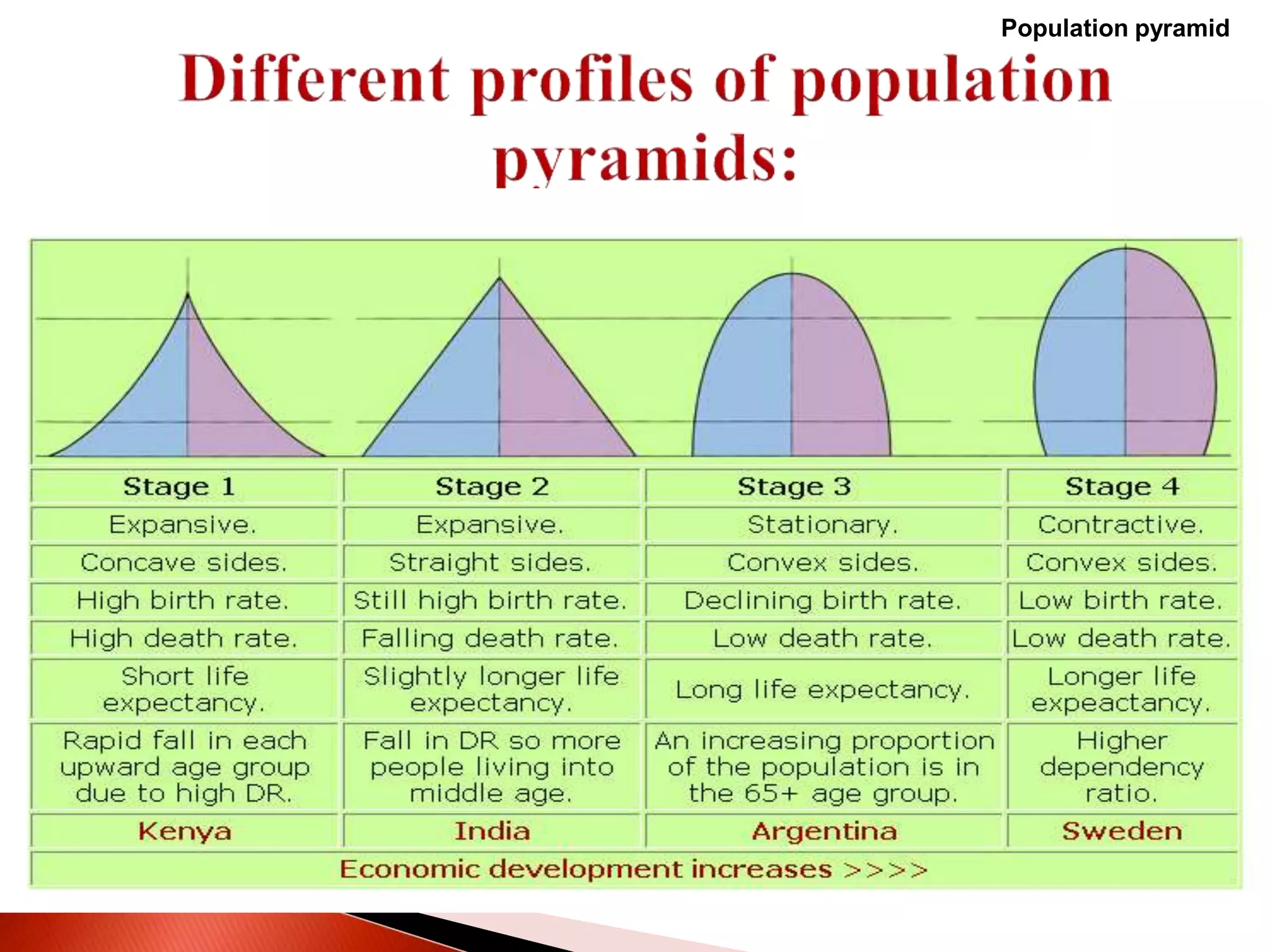
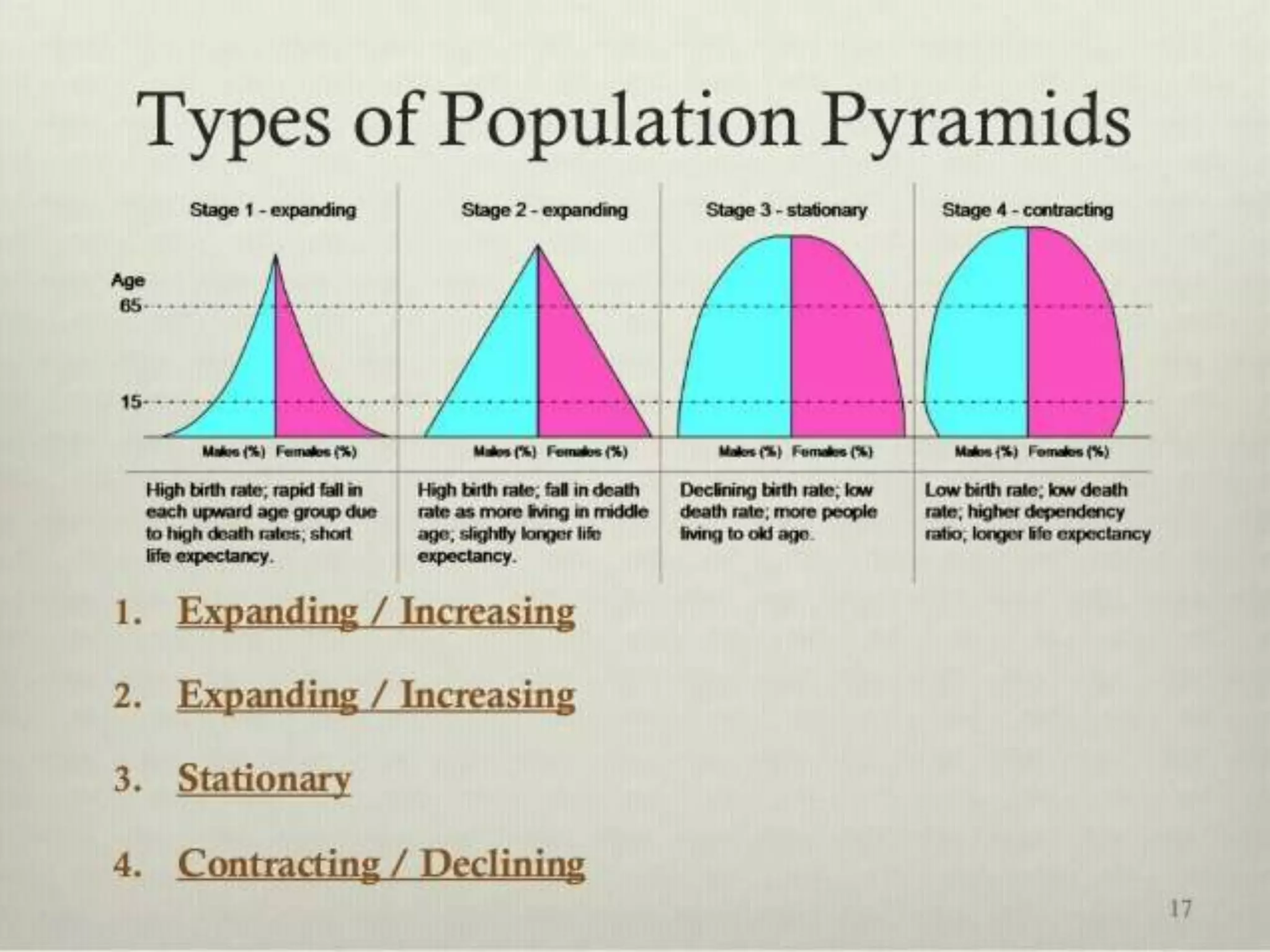
Describe & interpret different profiles of the
population pyramid
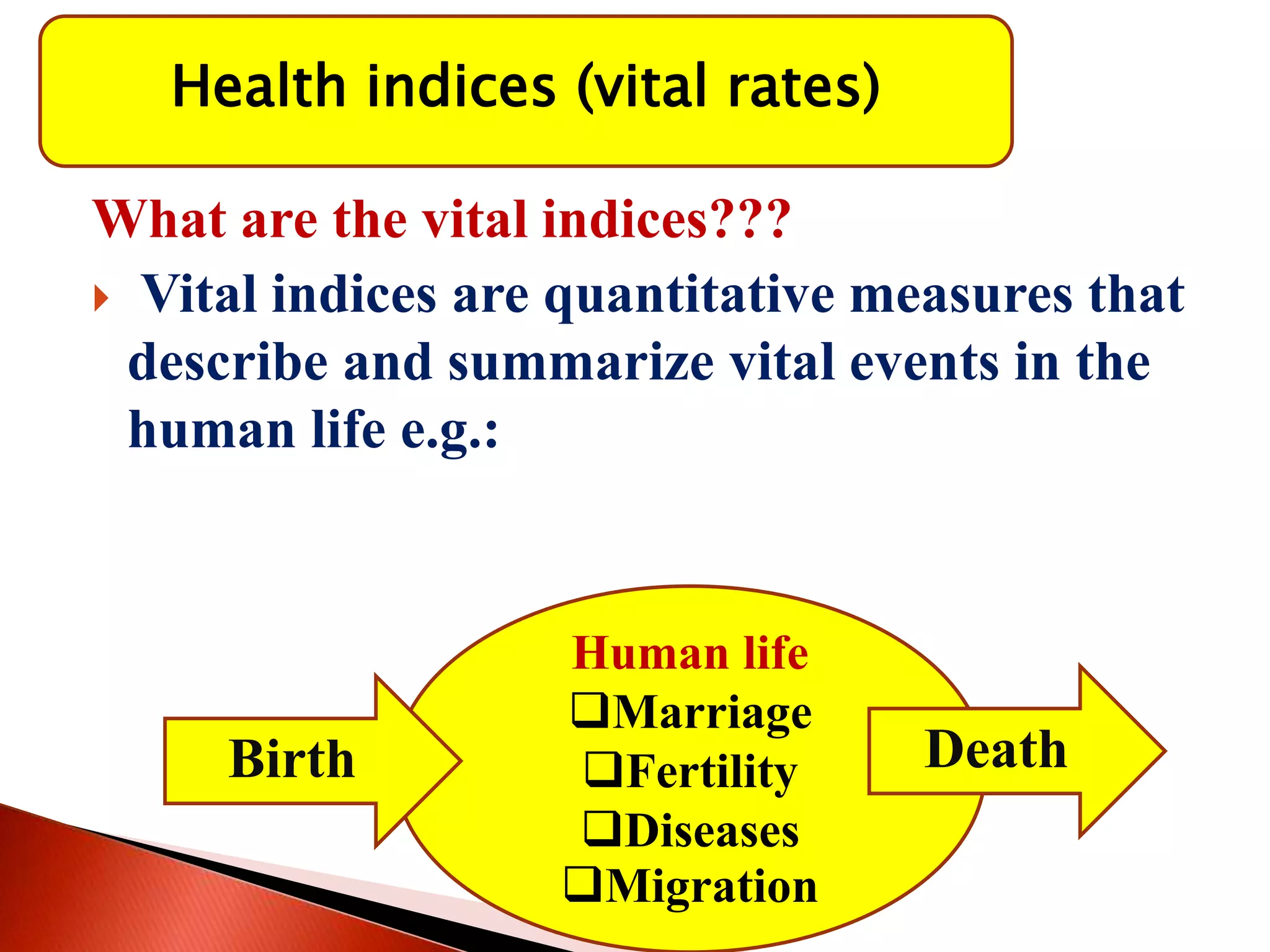
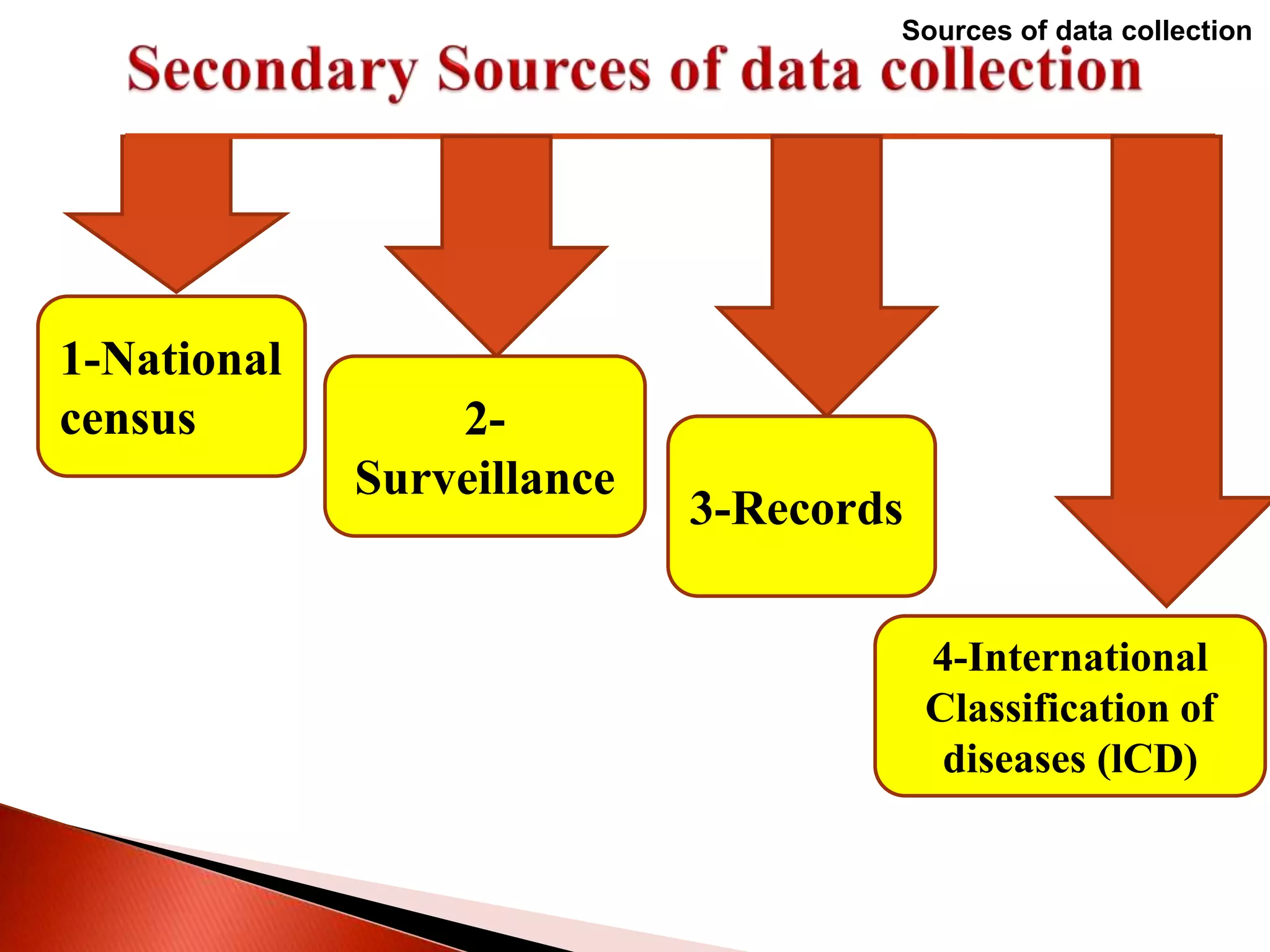
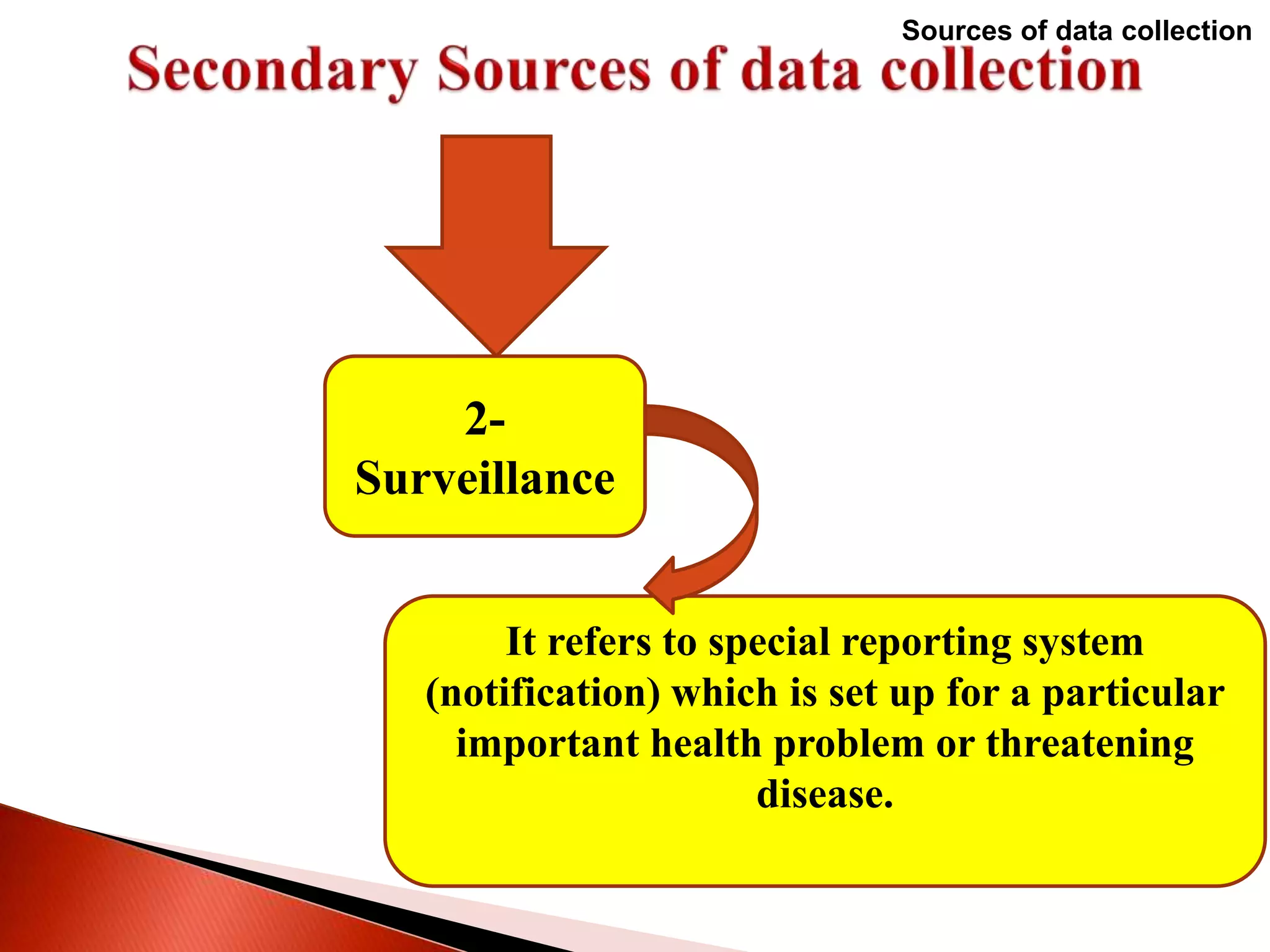
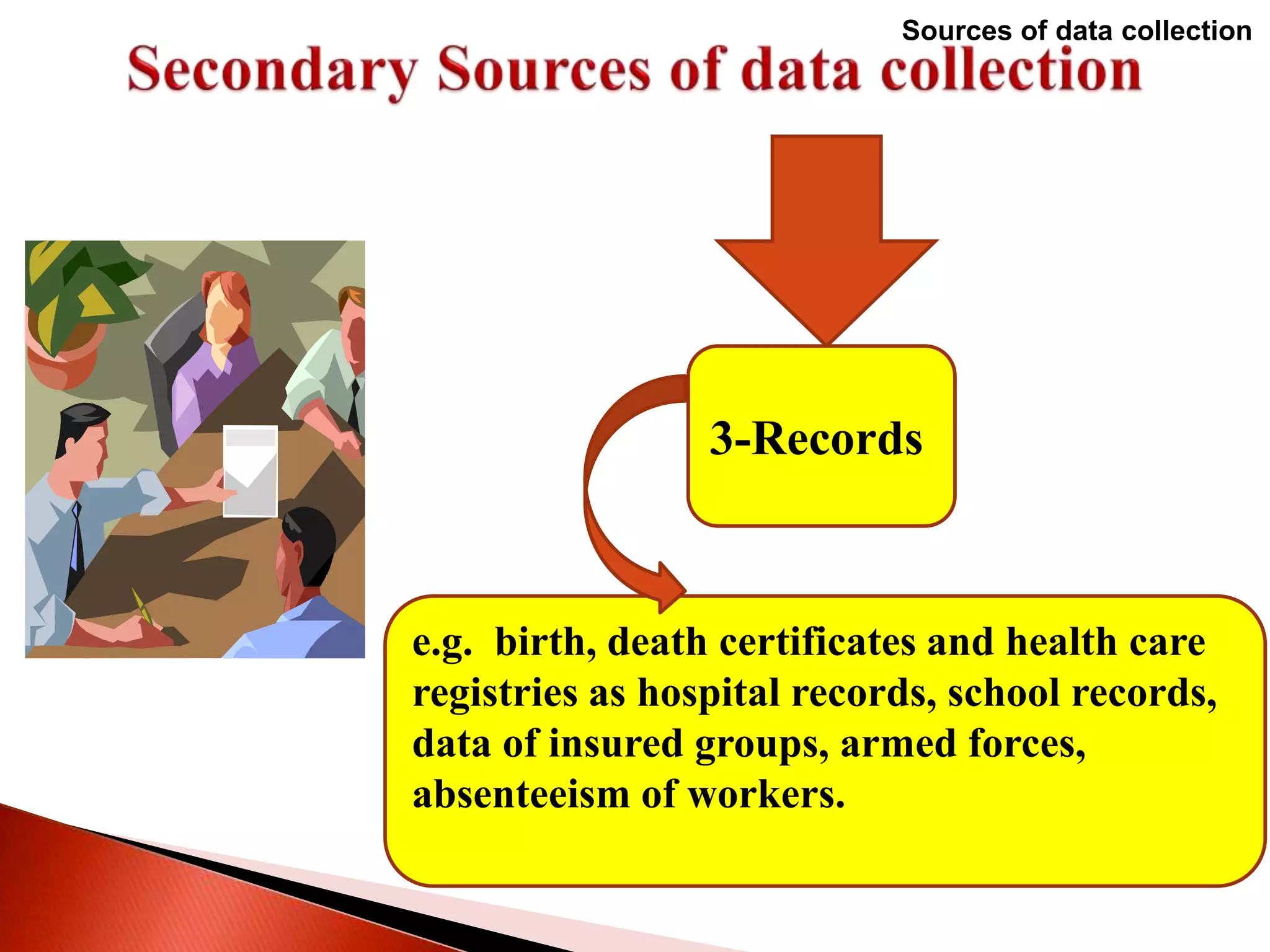
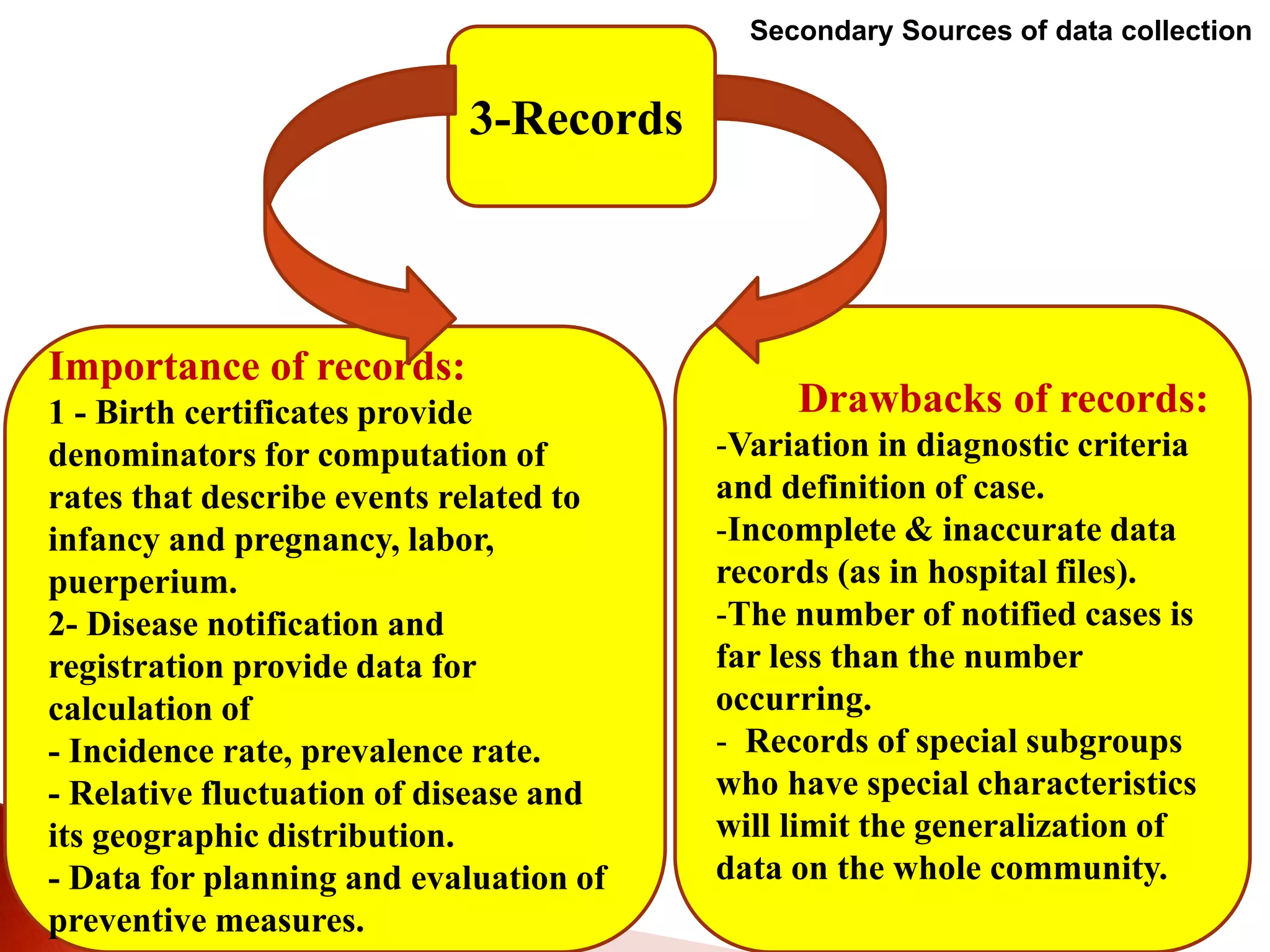
Categorize data sources for vital statistics
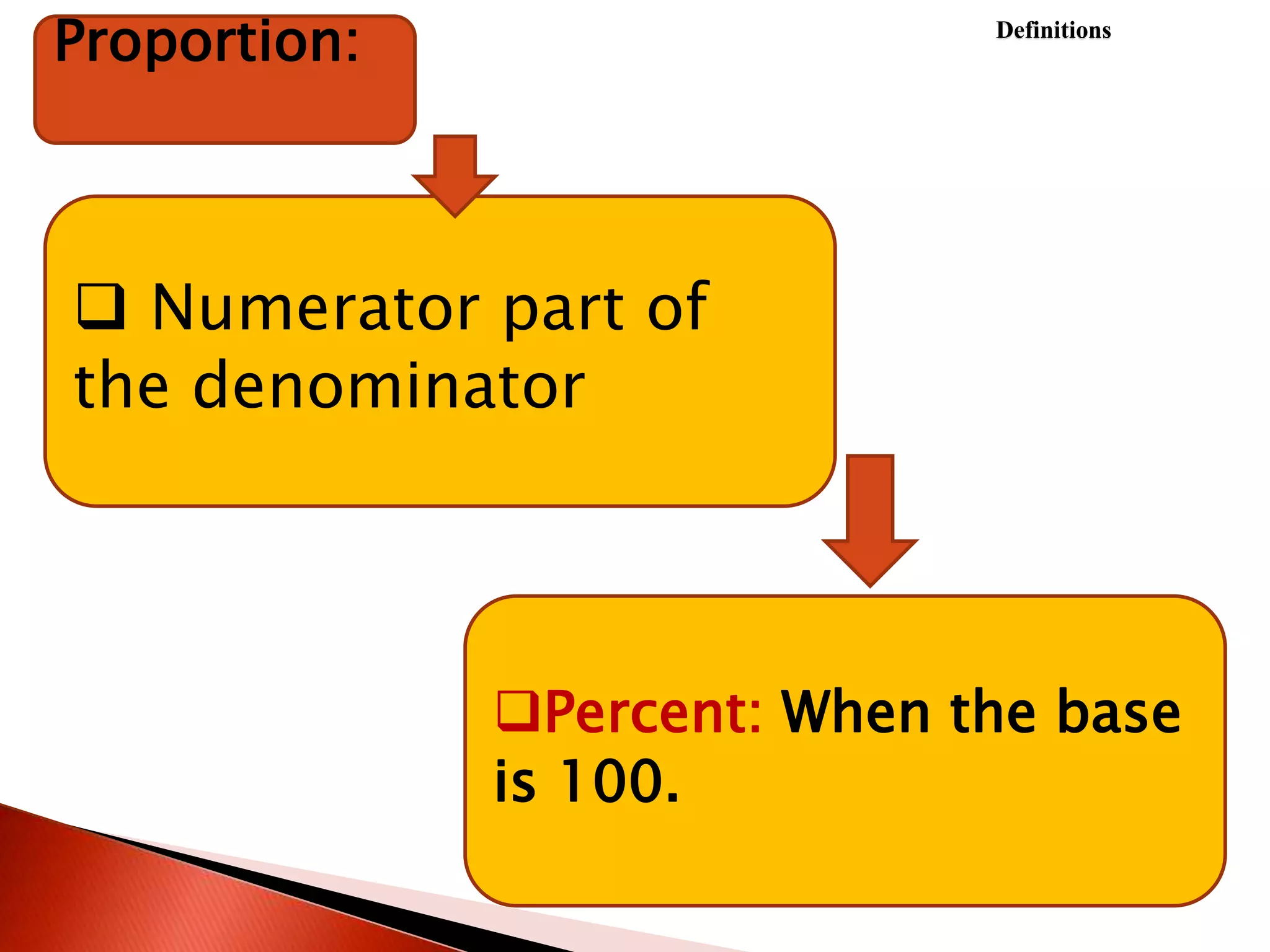
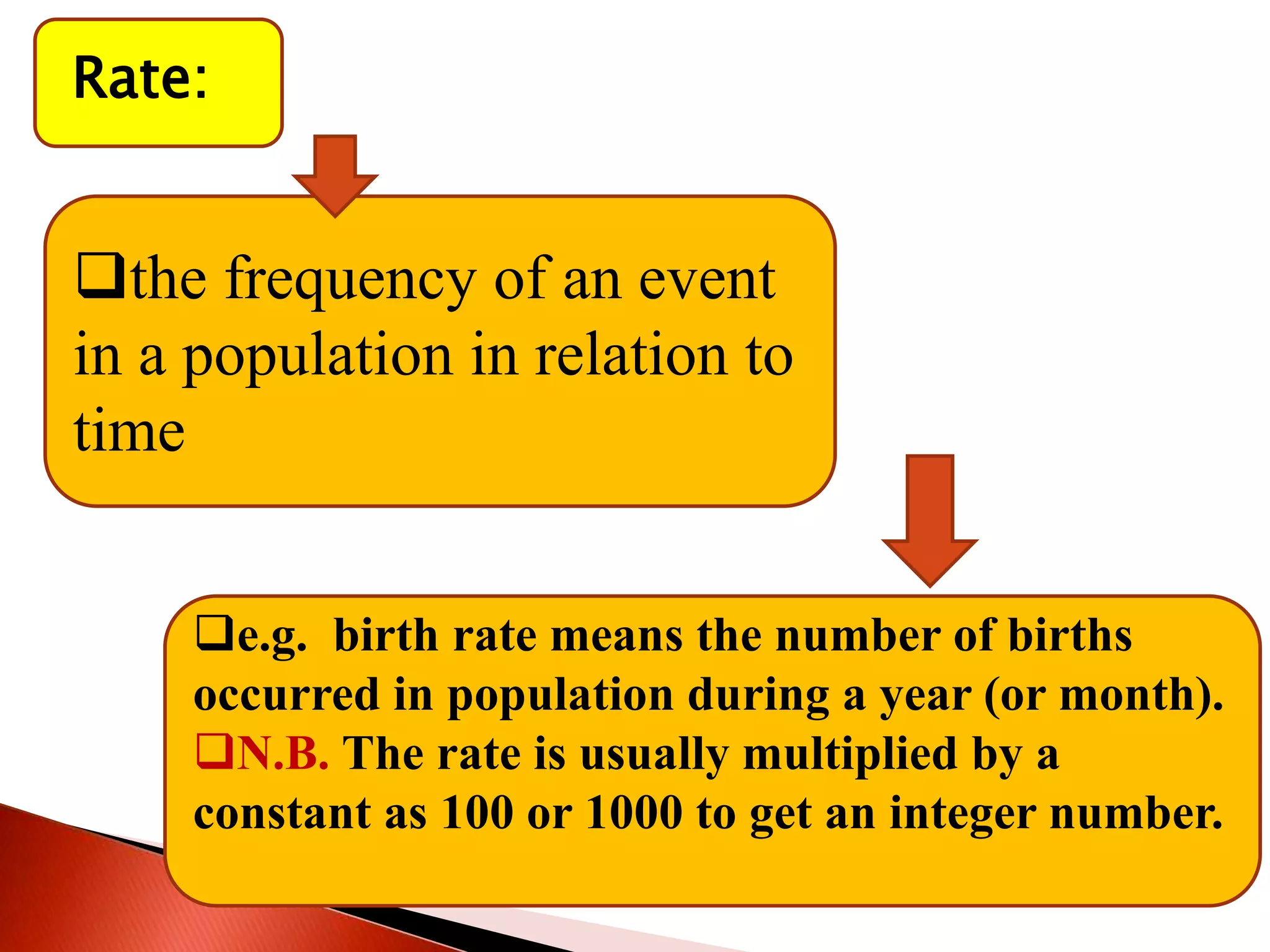
Differentiate between proportion, ratio, and rate.
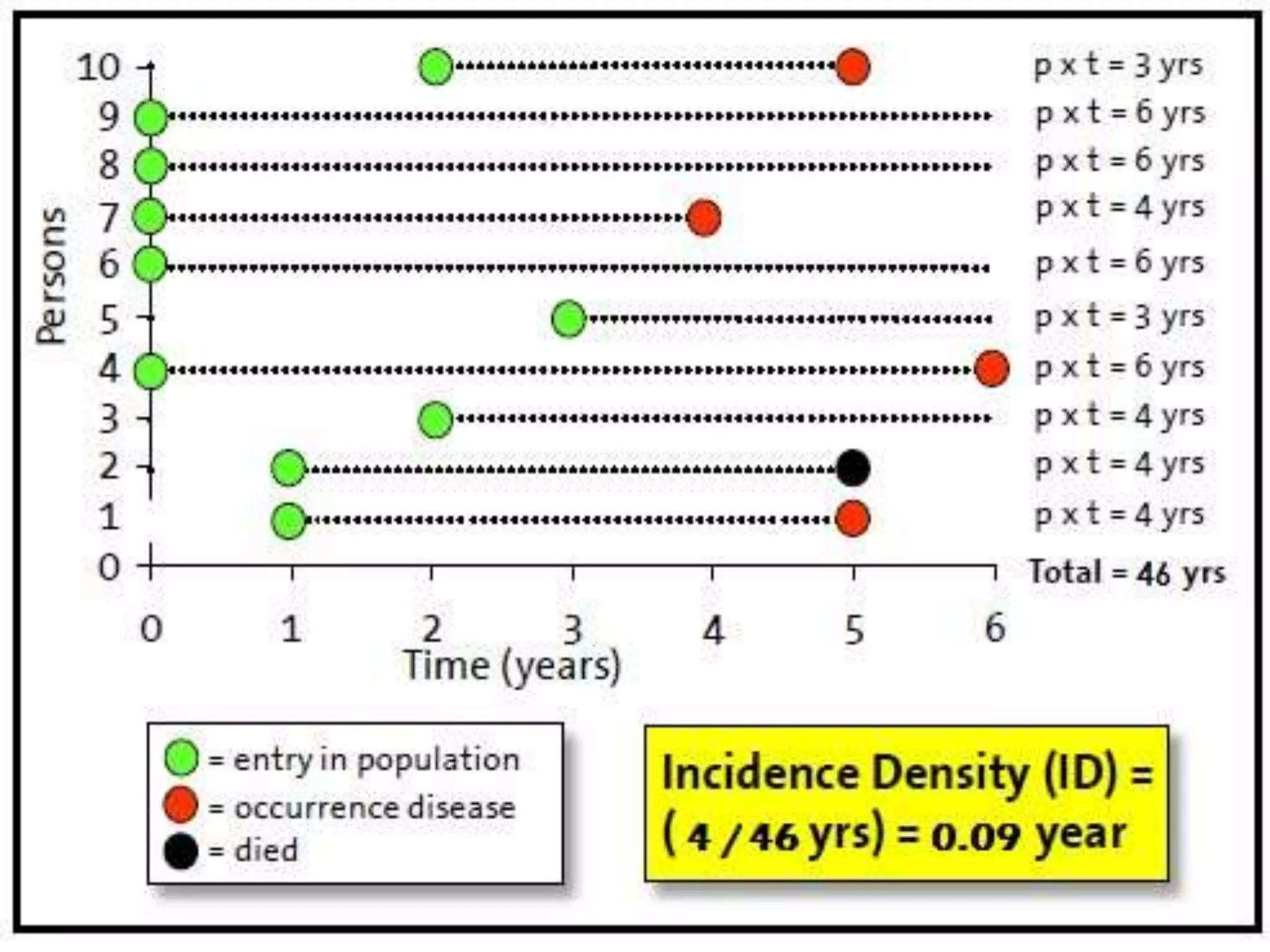
Calculate Vital indices [fertility - birth, morbidity
(disease) –death (mortality)].
Recognize the relationship between MDGS & vital
indices](https://image.slidesharecdn.com/demography-updated-230131163014-c5d45485/75/demography-2-2048.jpg)