
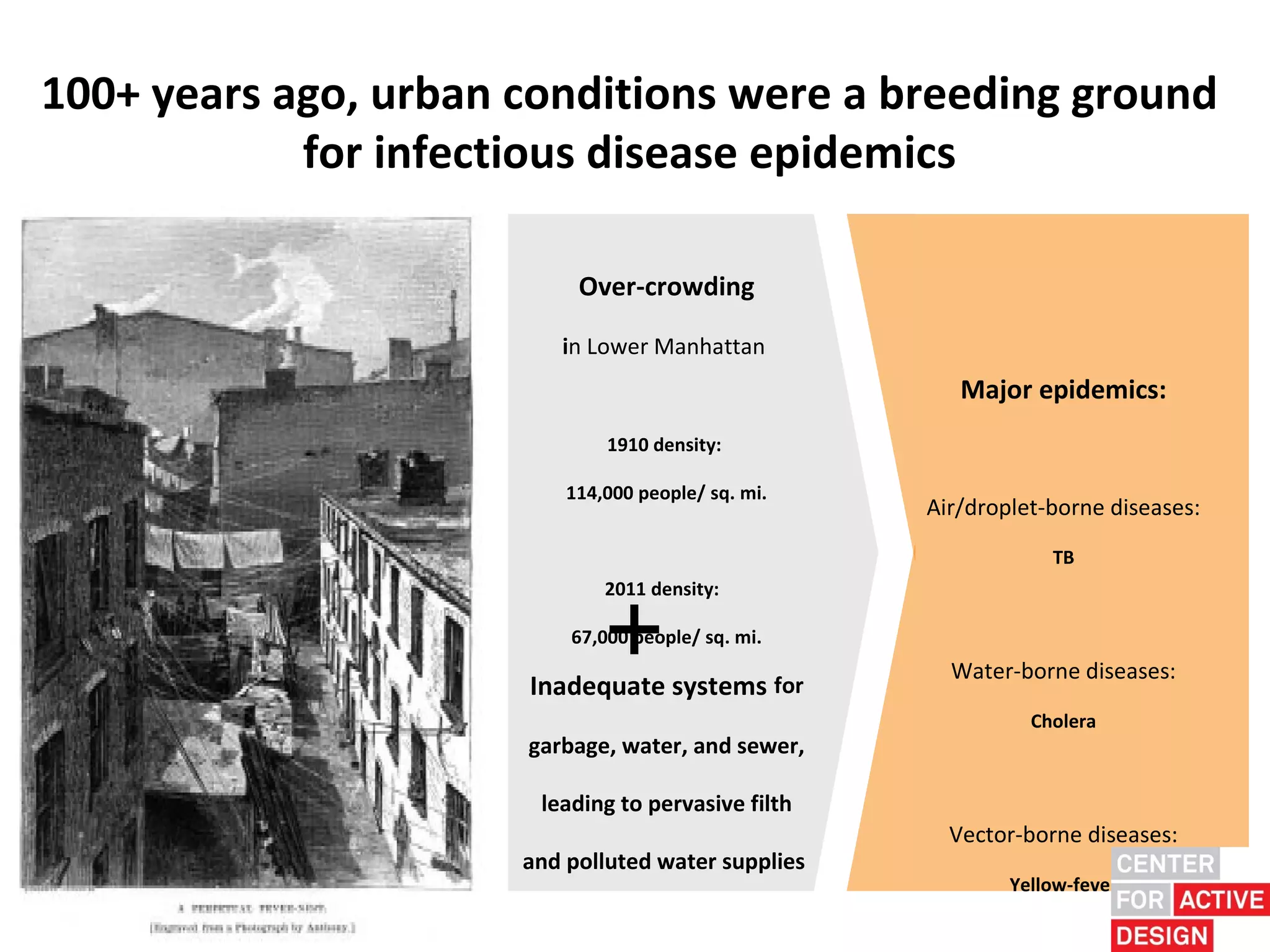
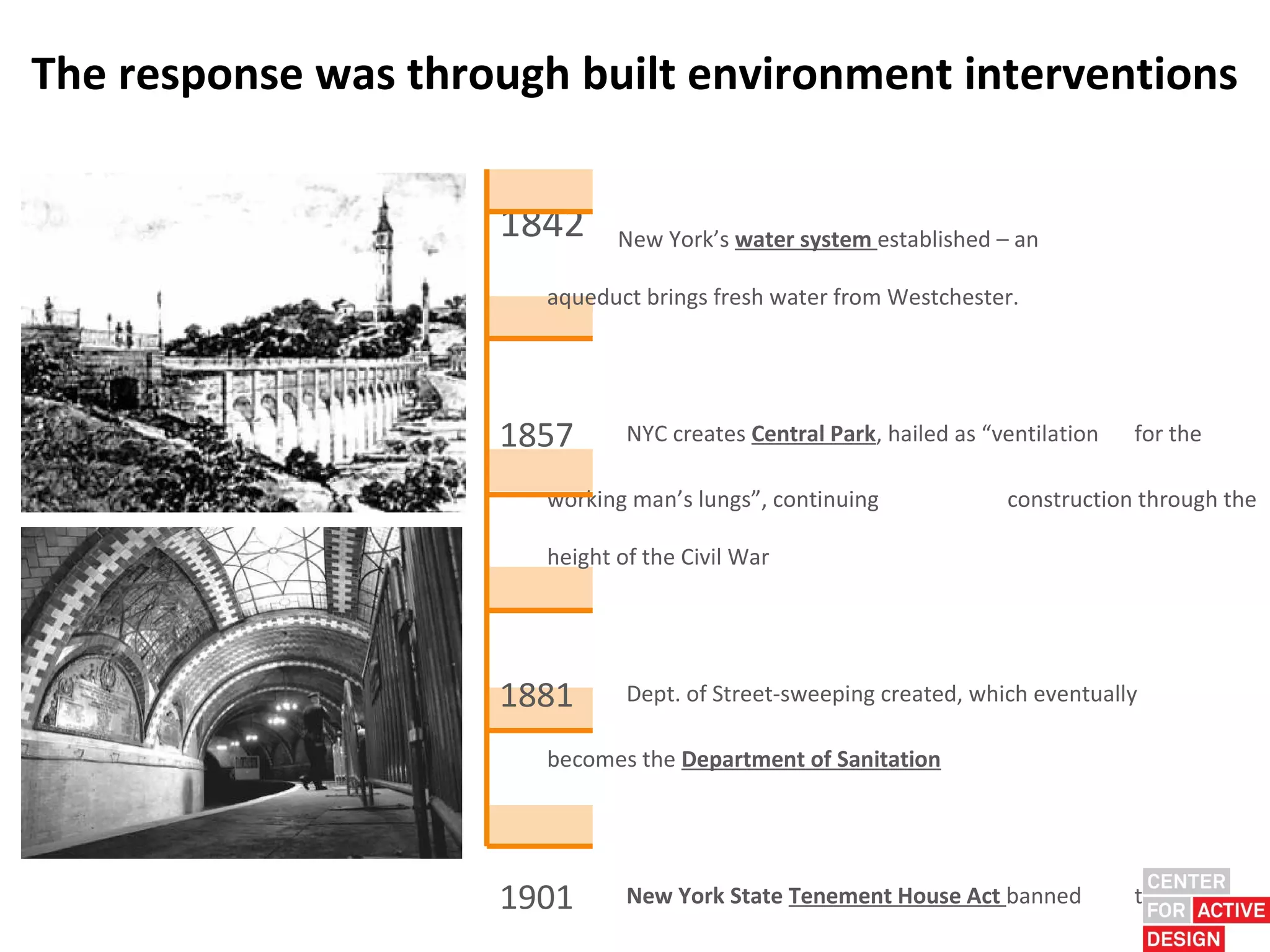
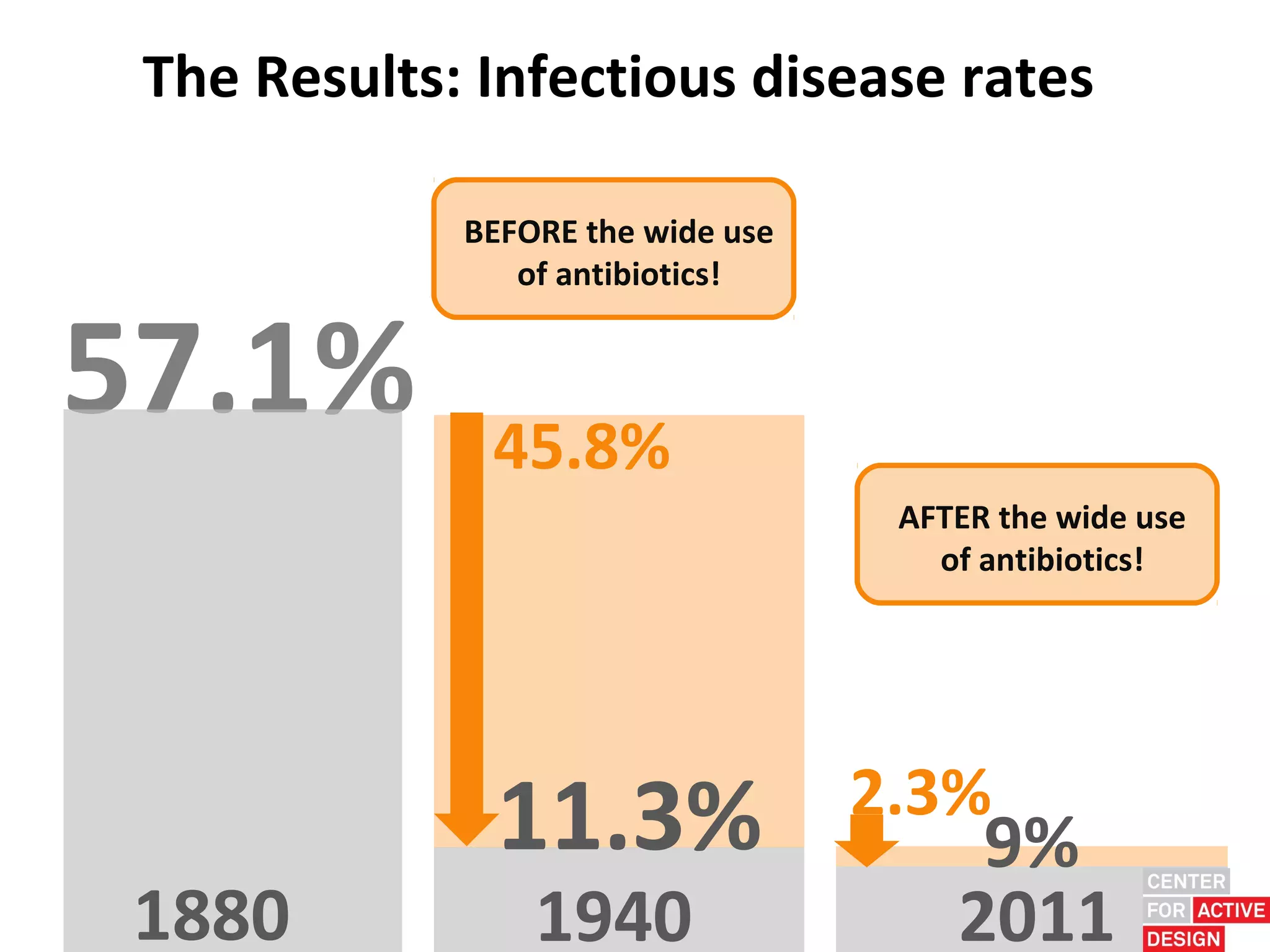
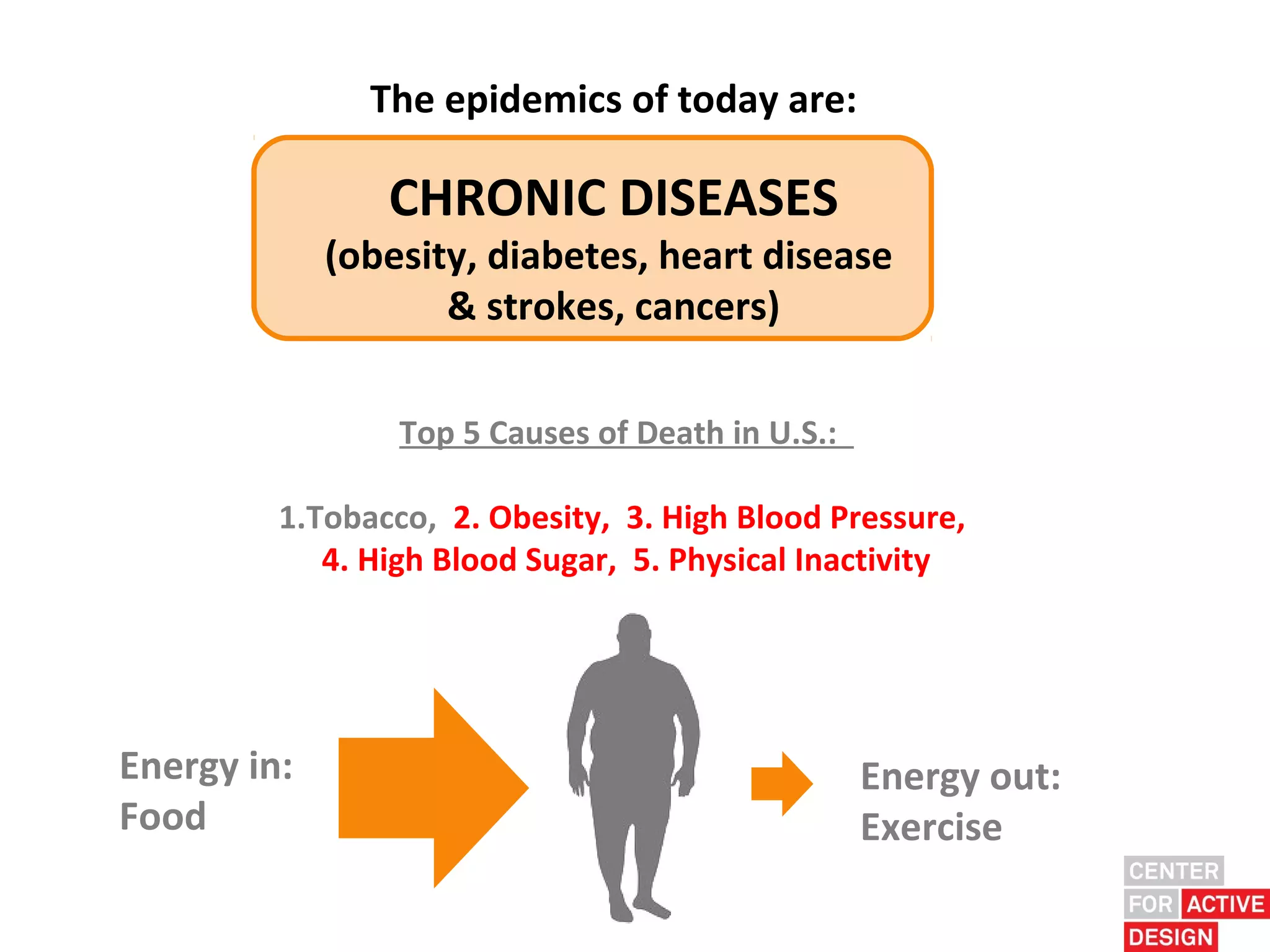
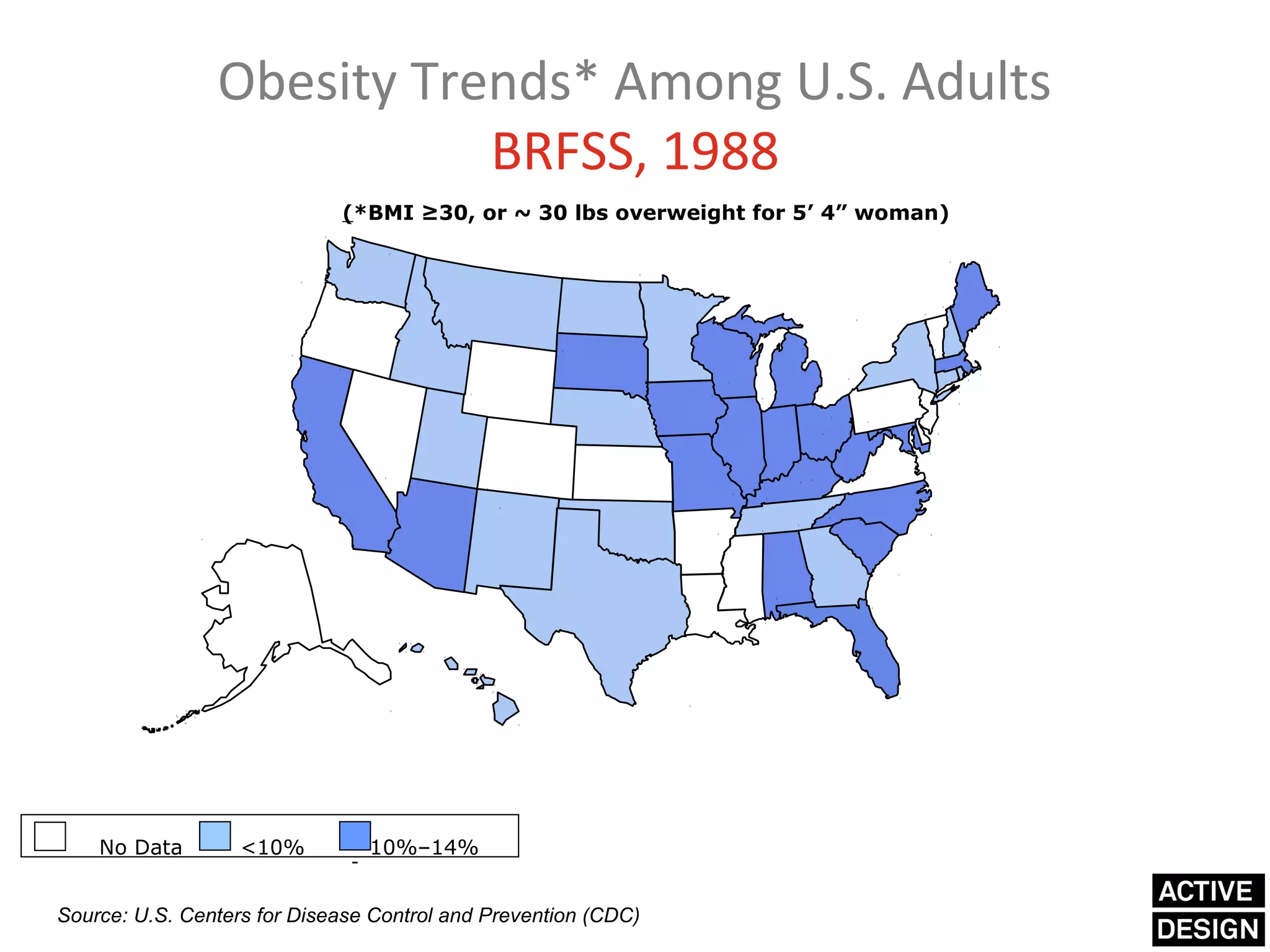
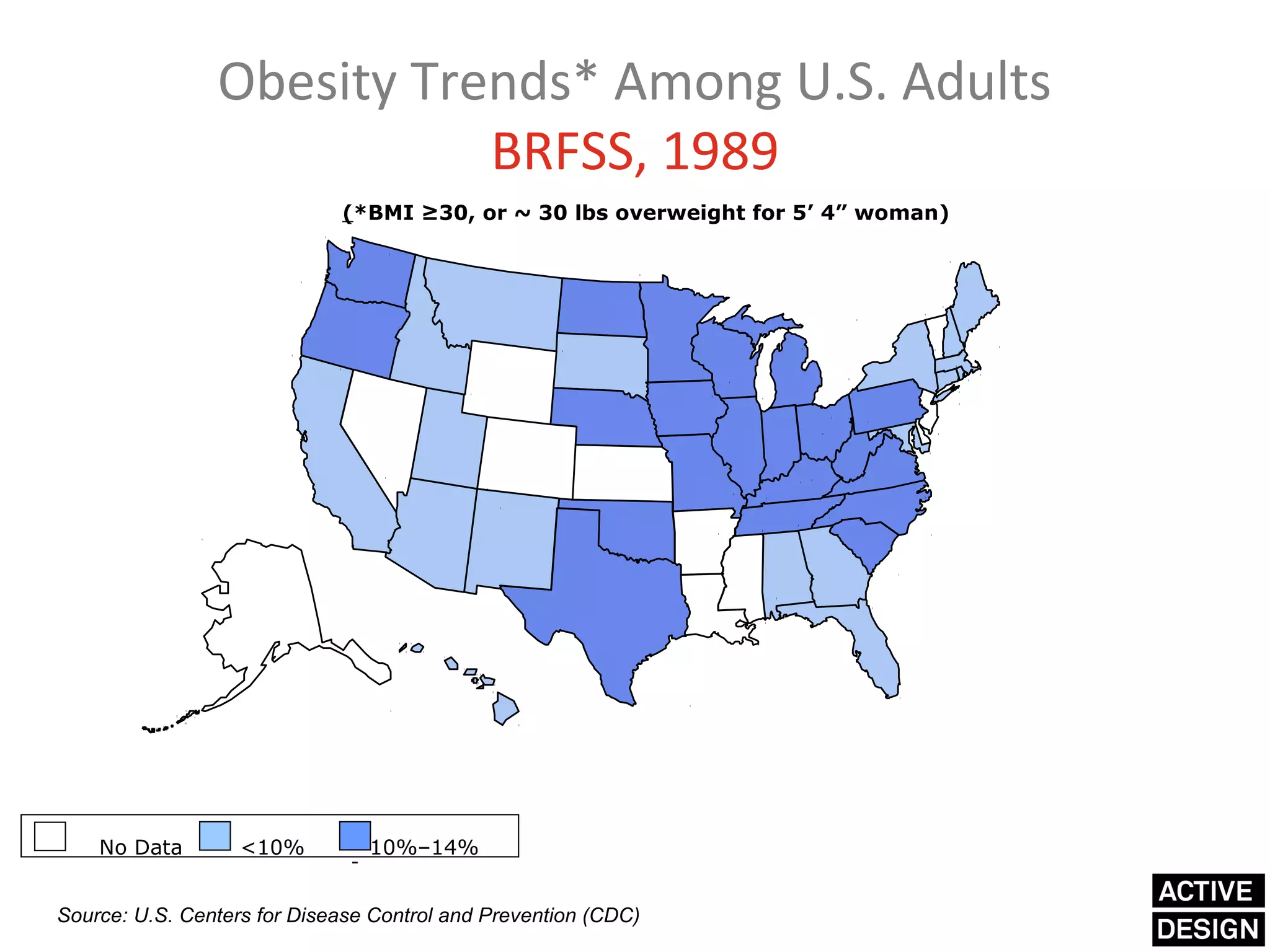
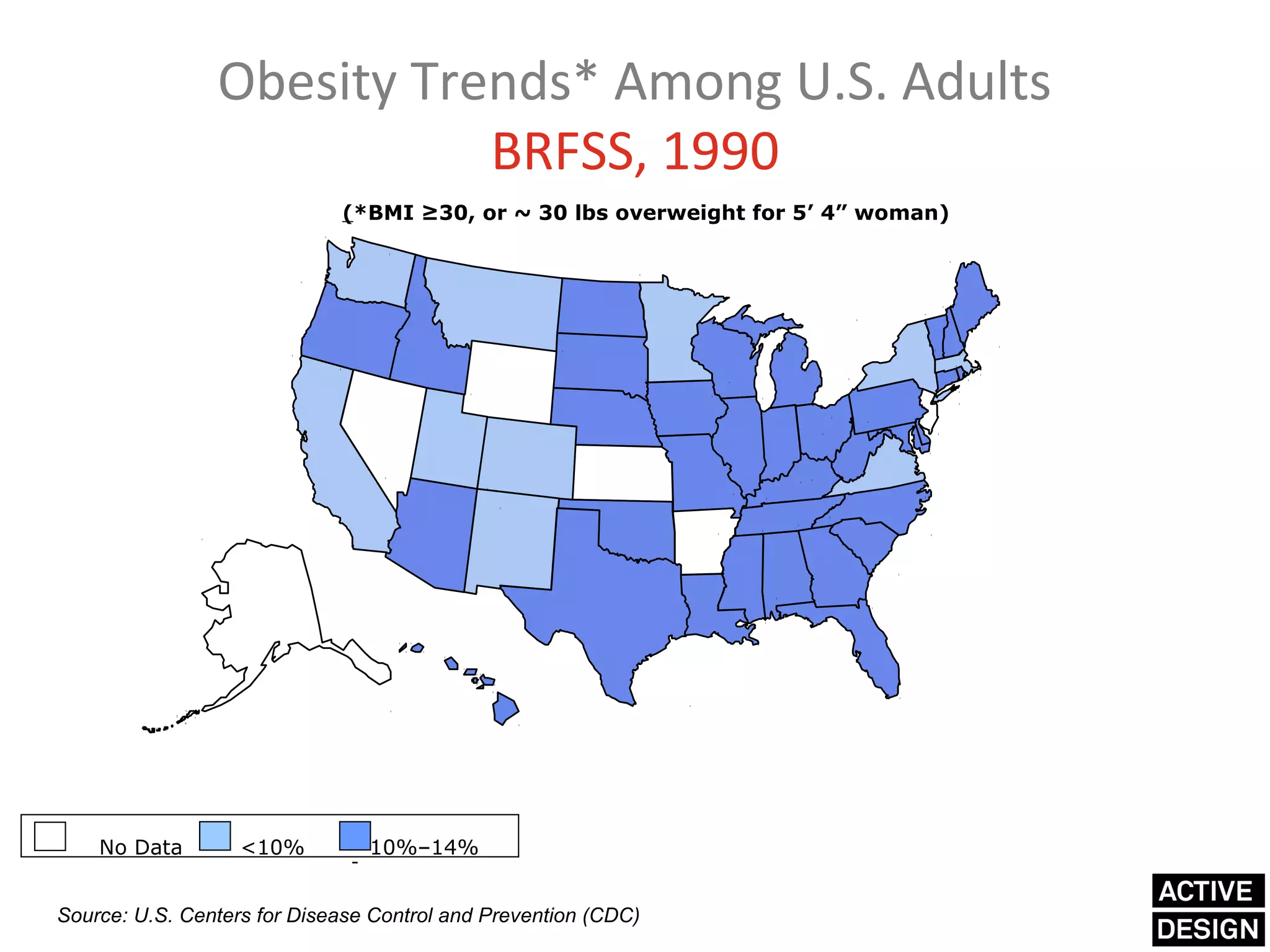
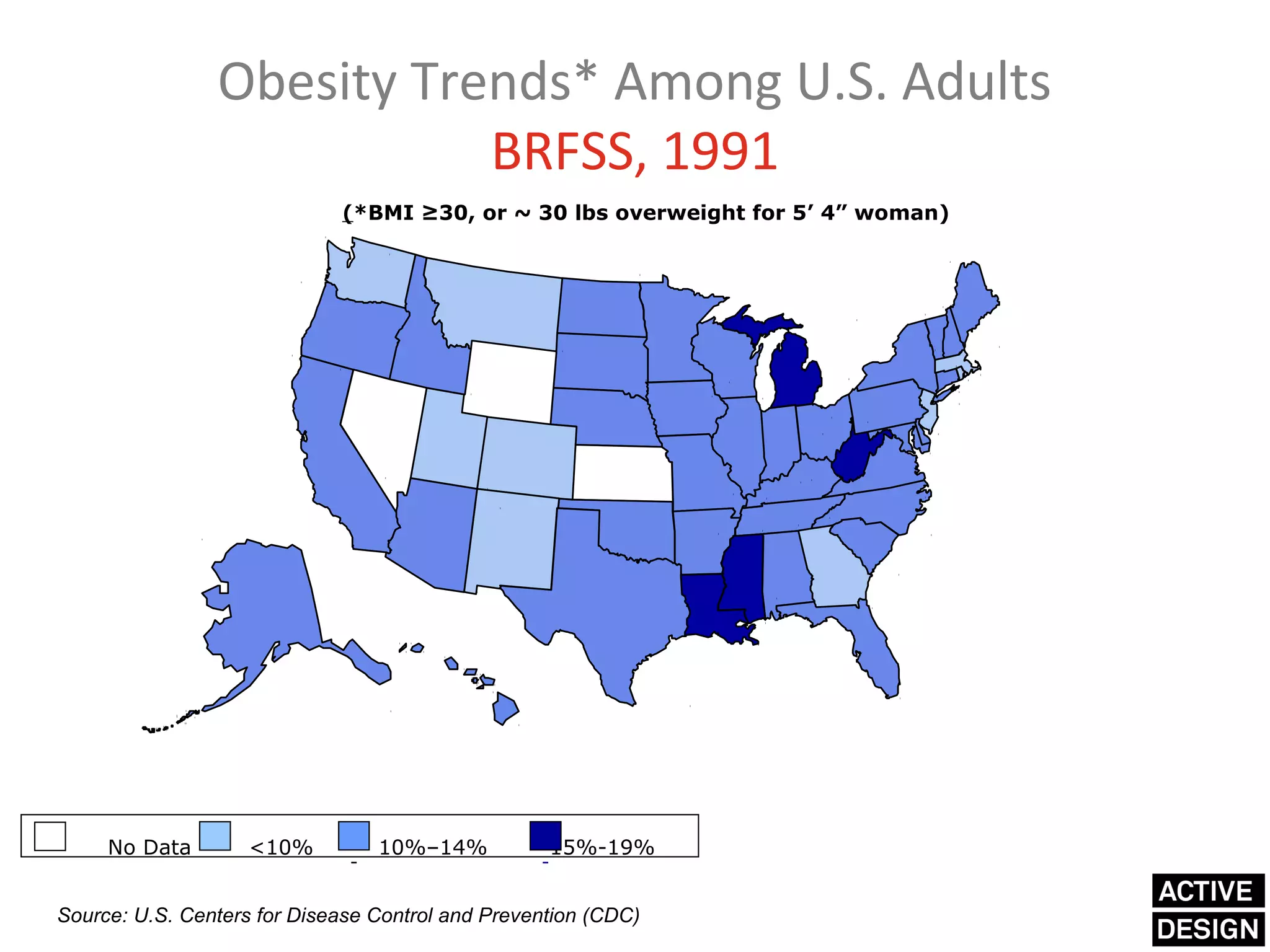
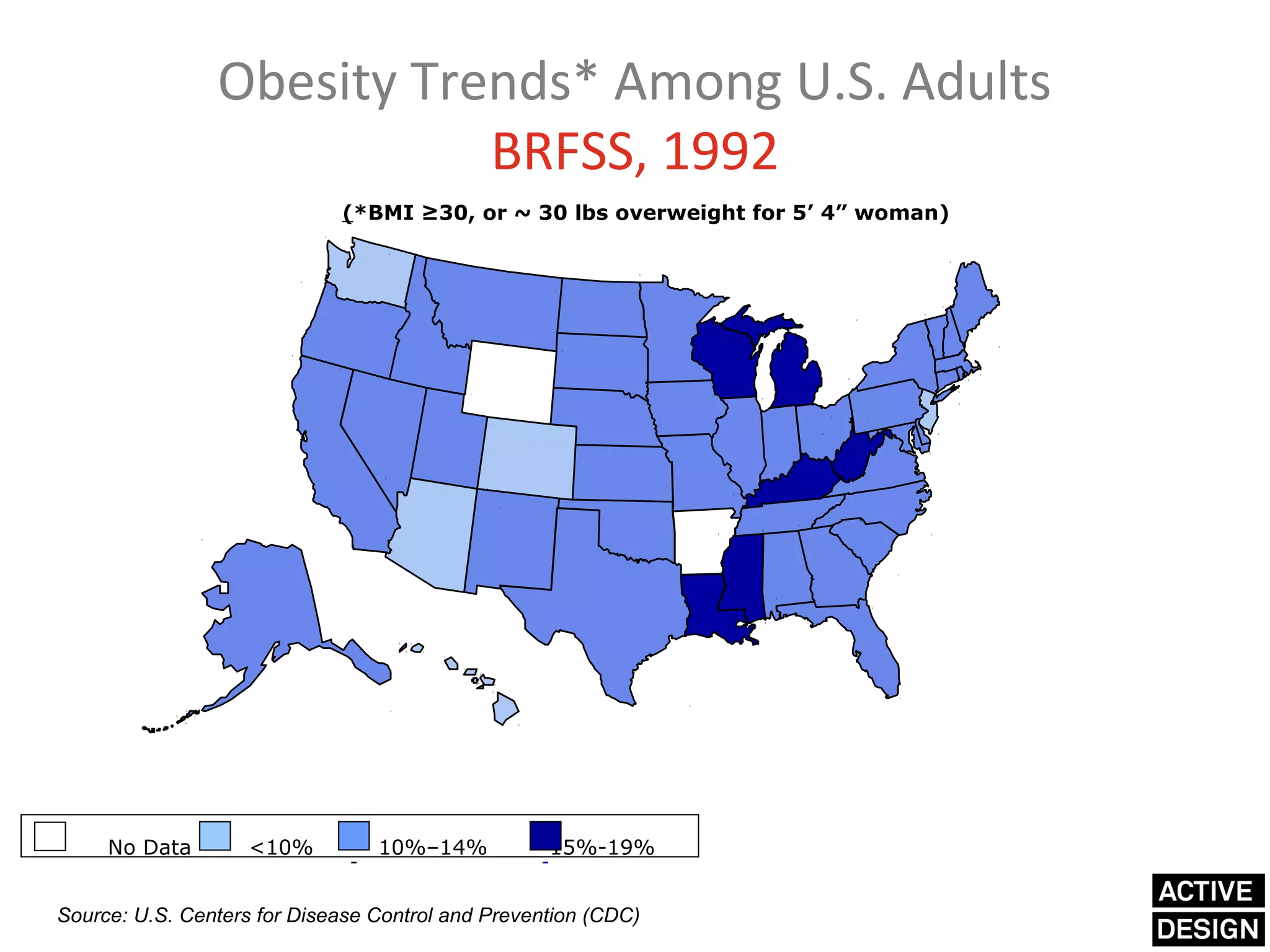
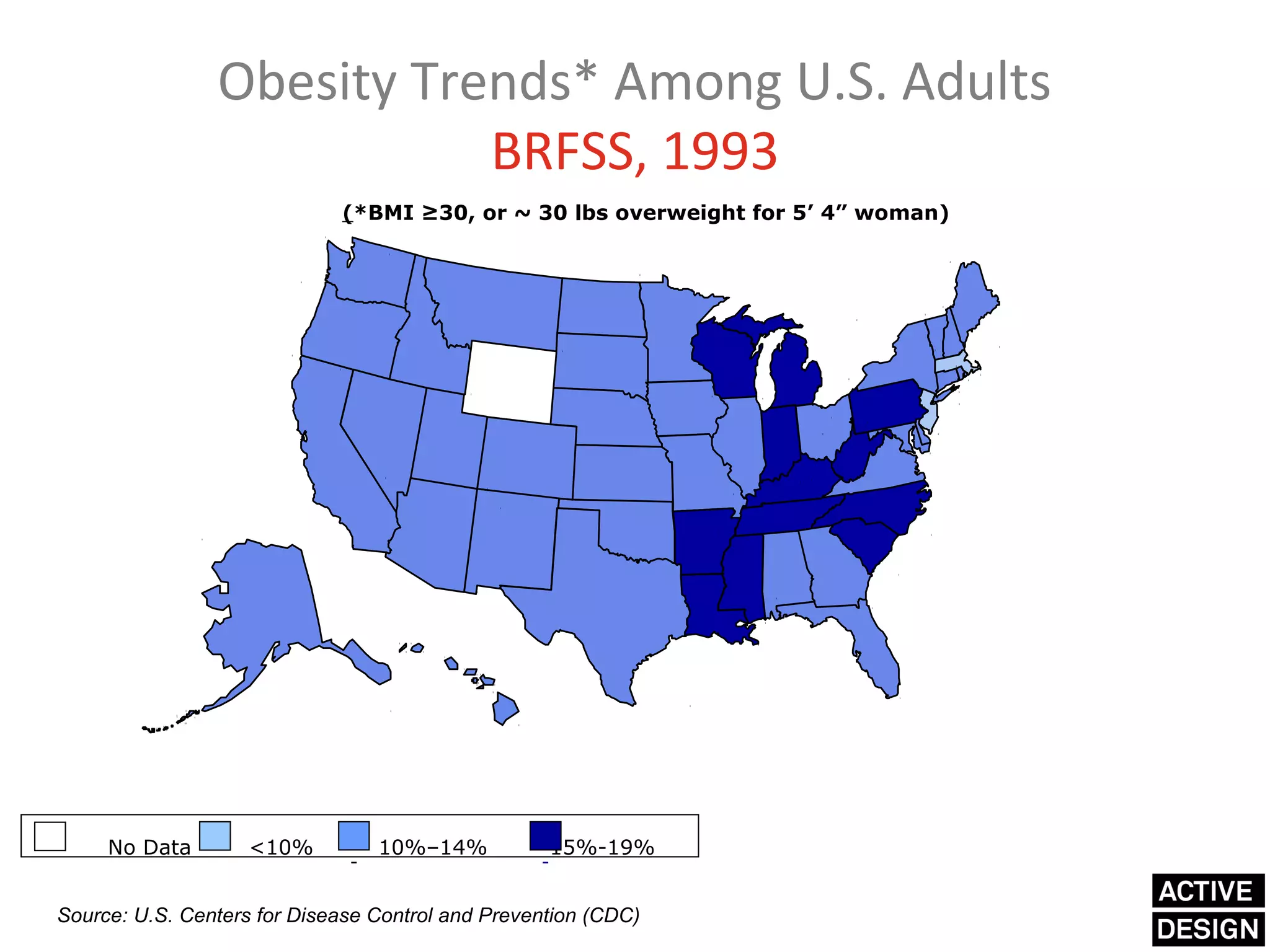
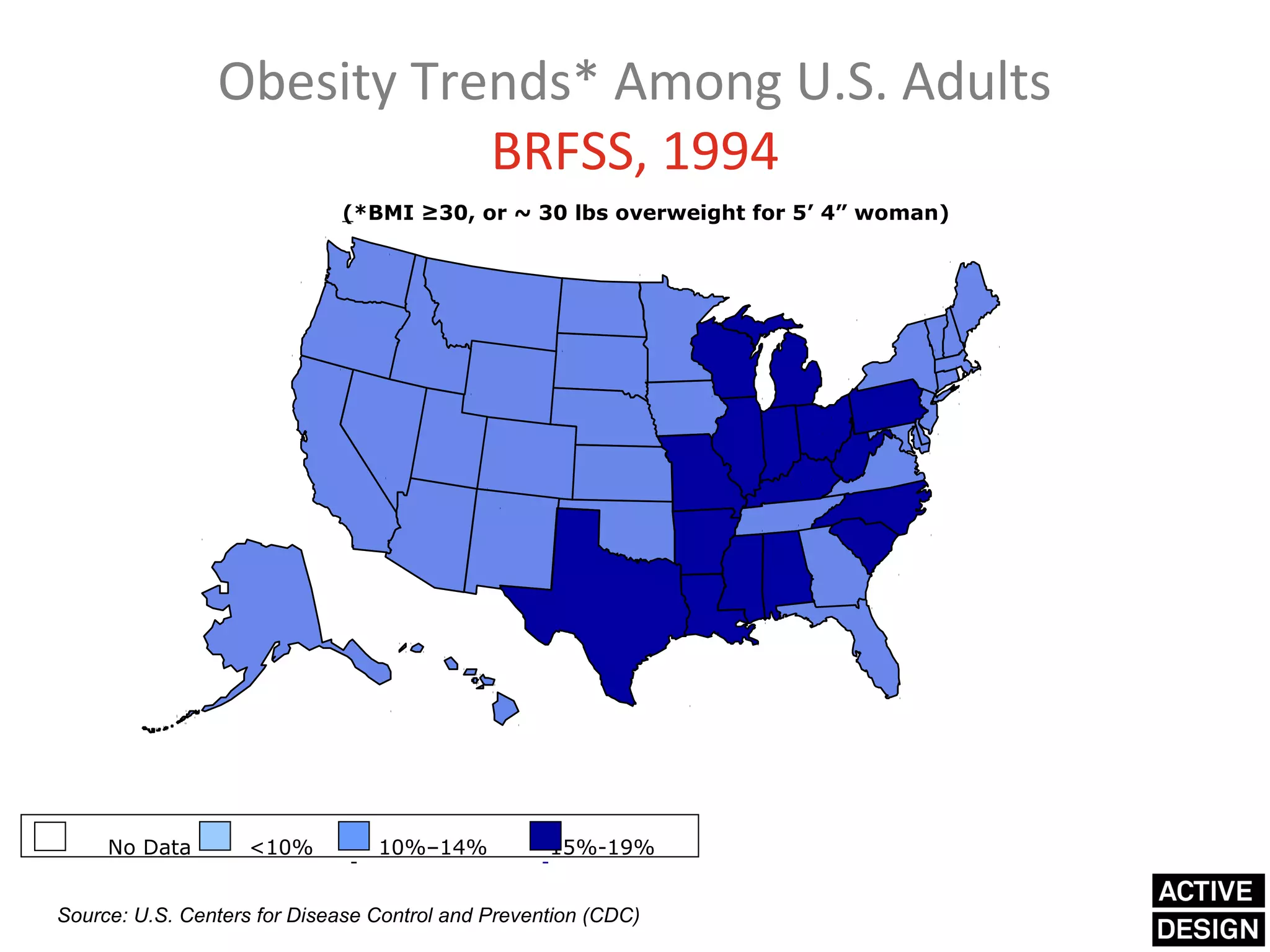
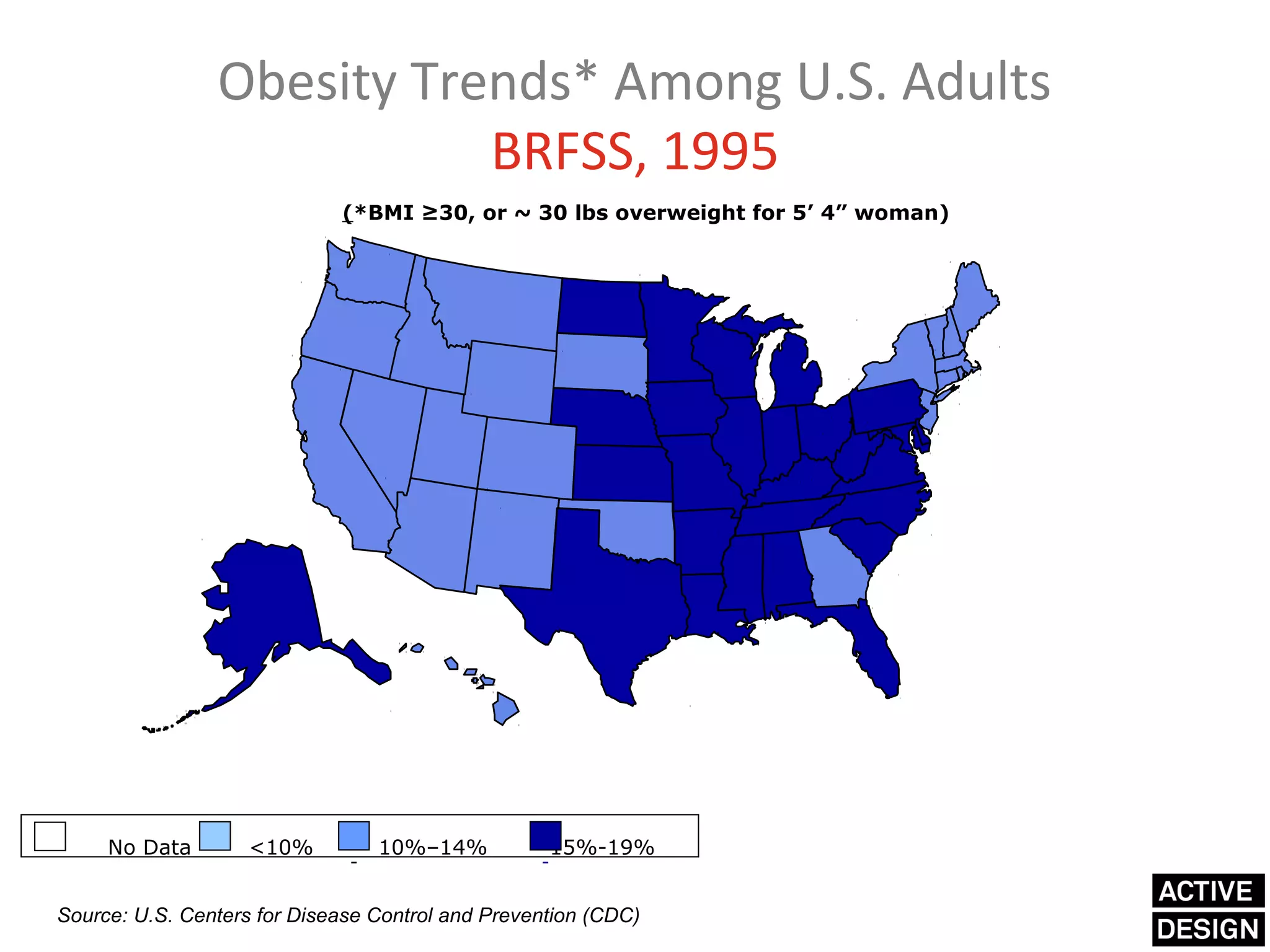
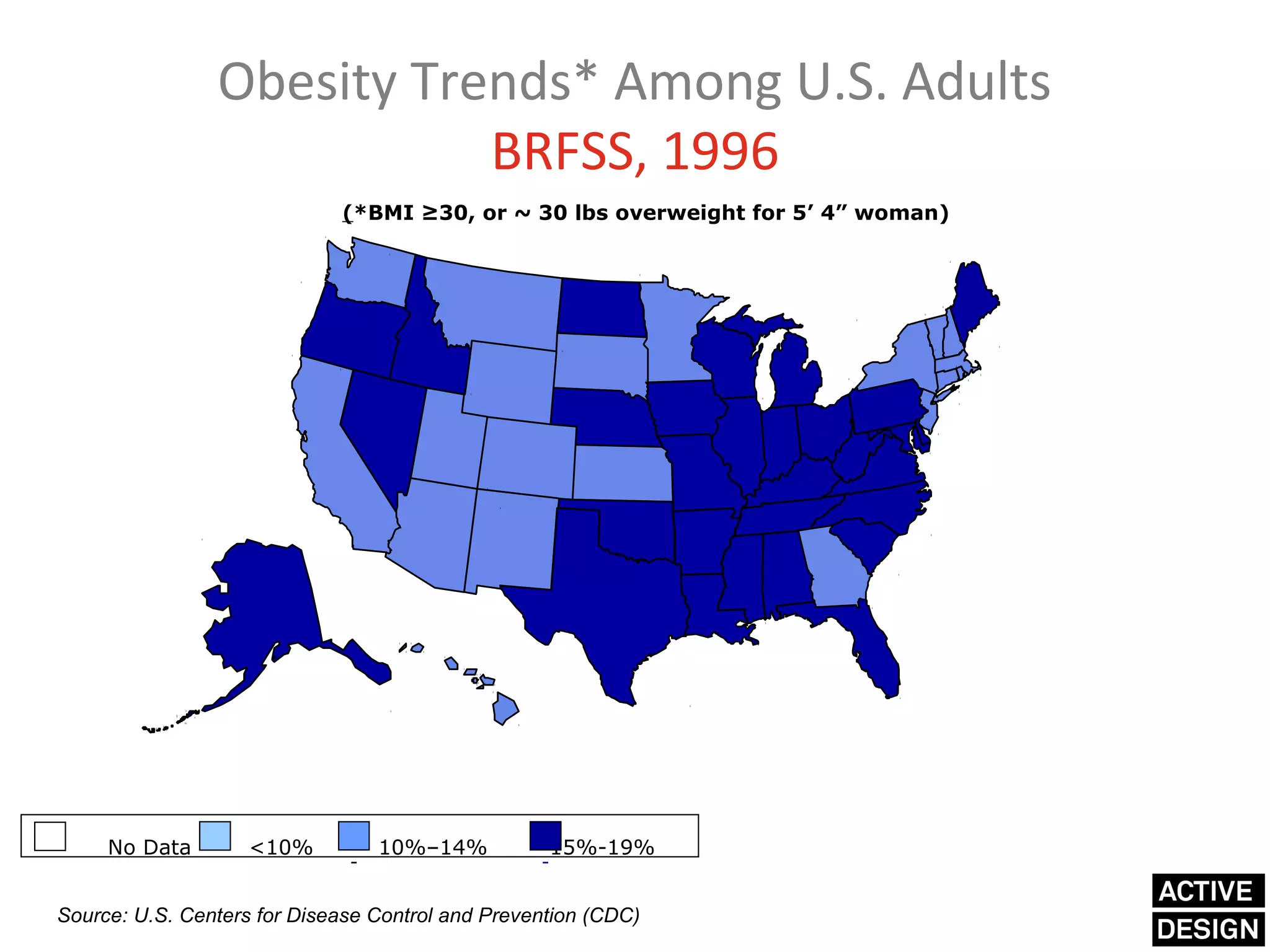
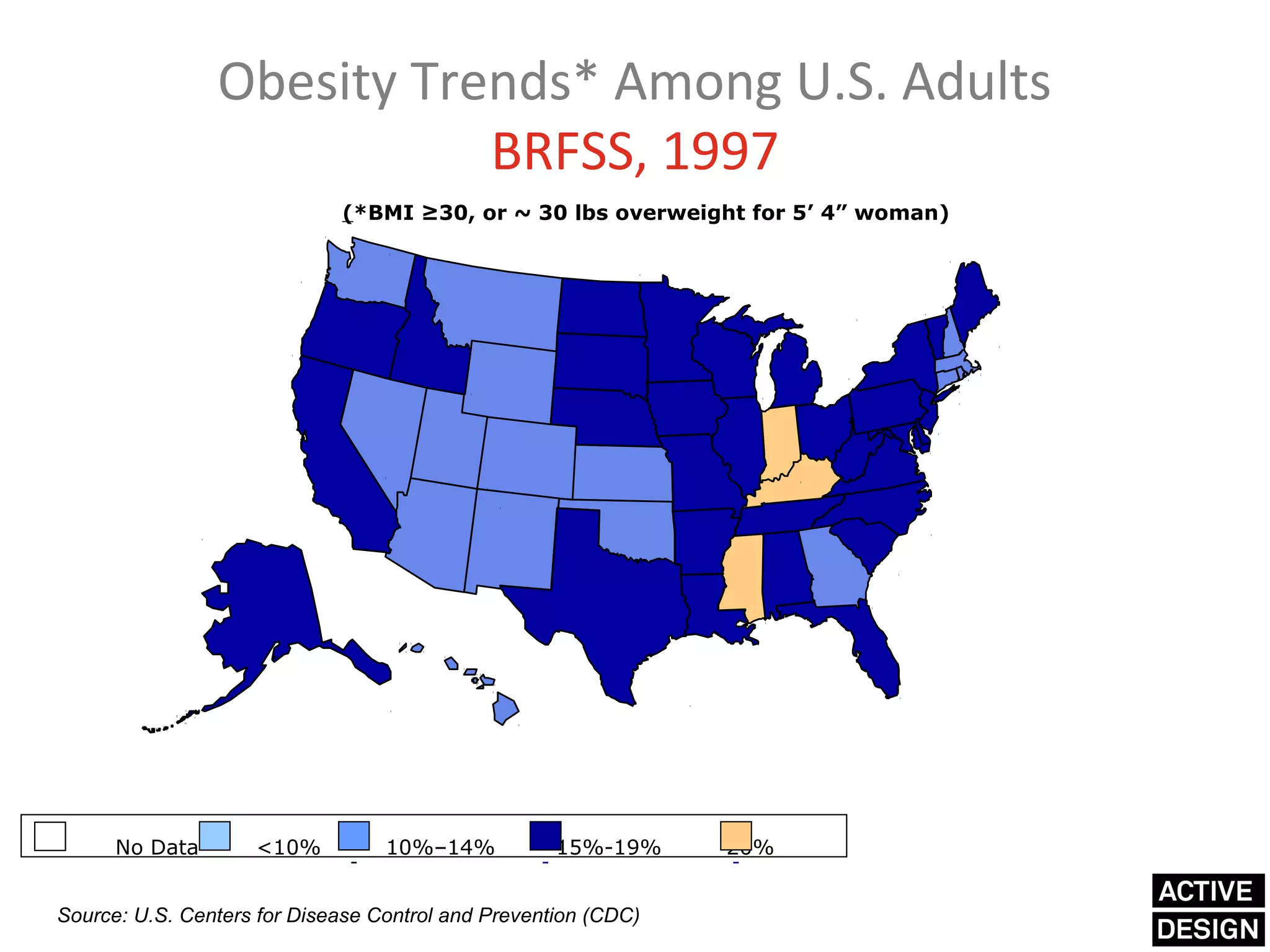
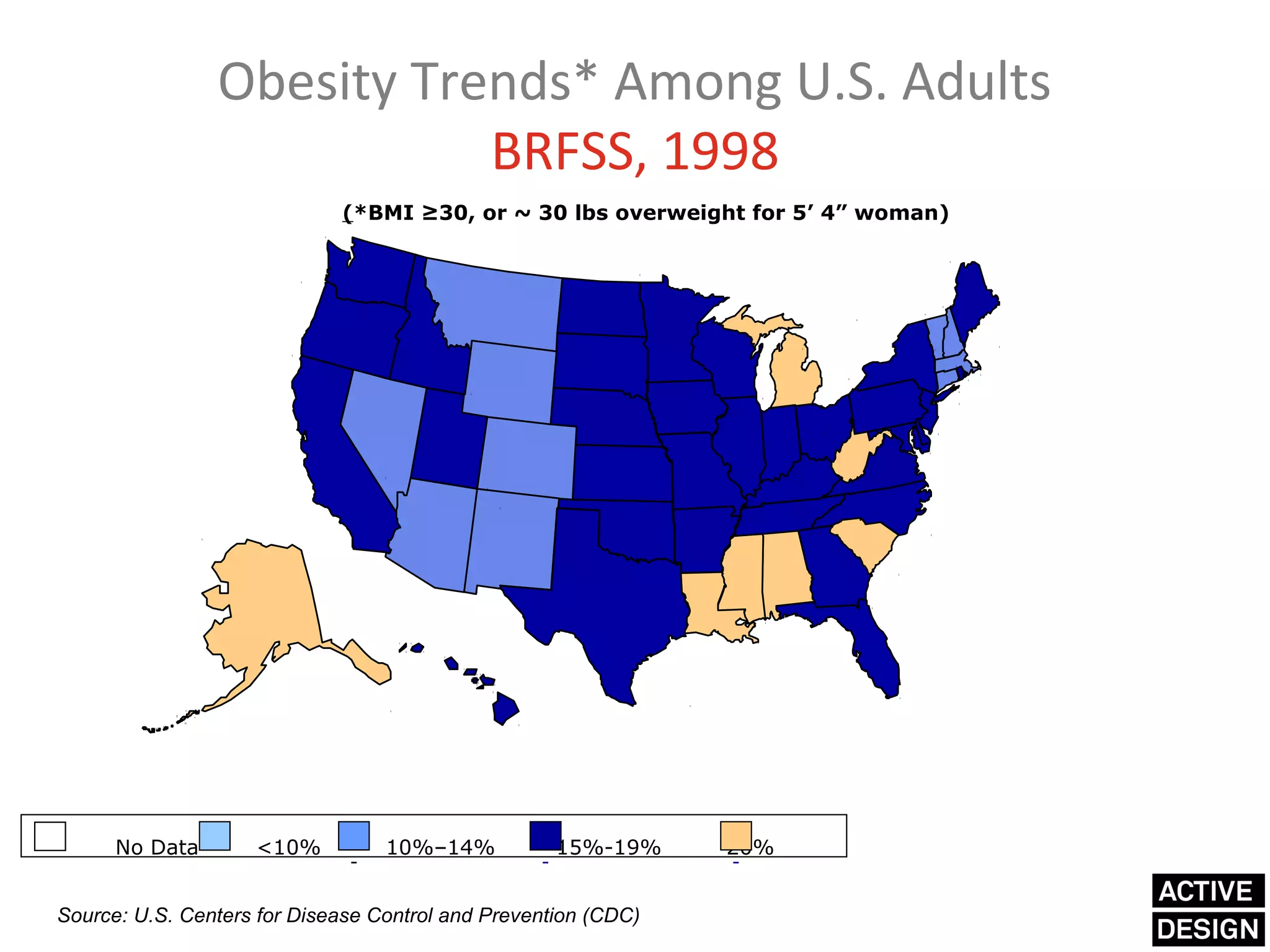
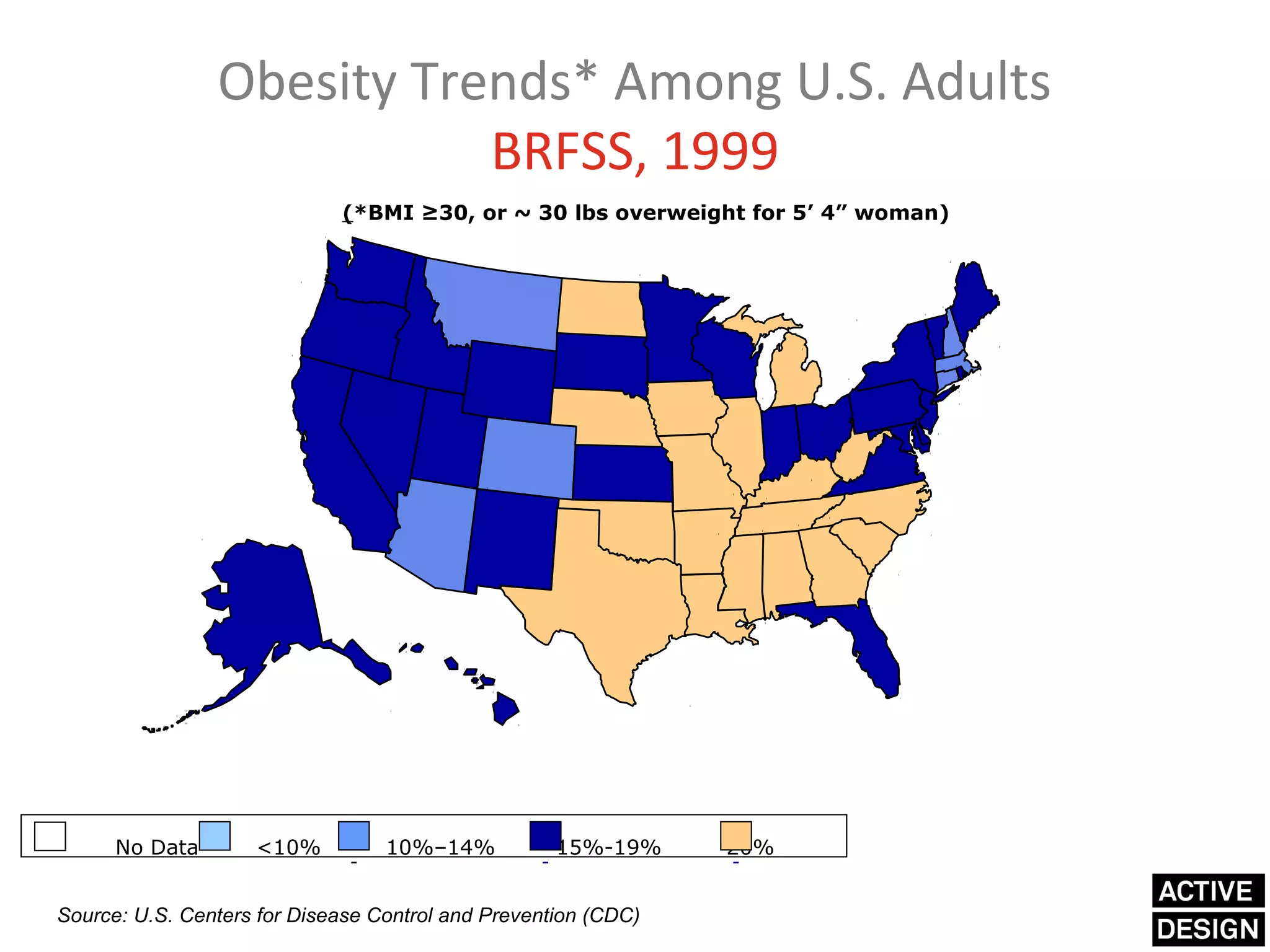
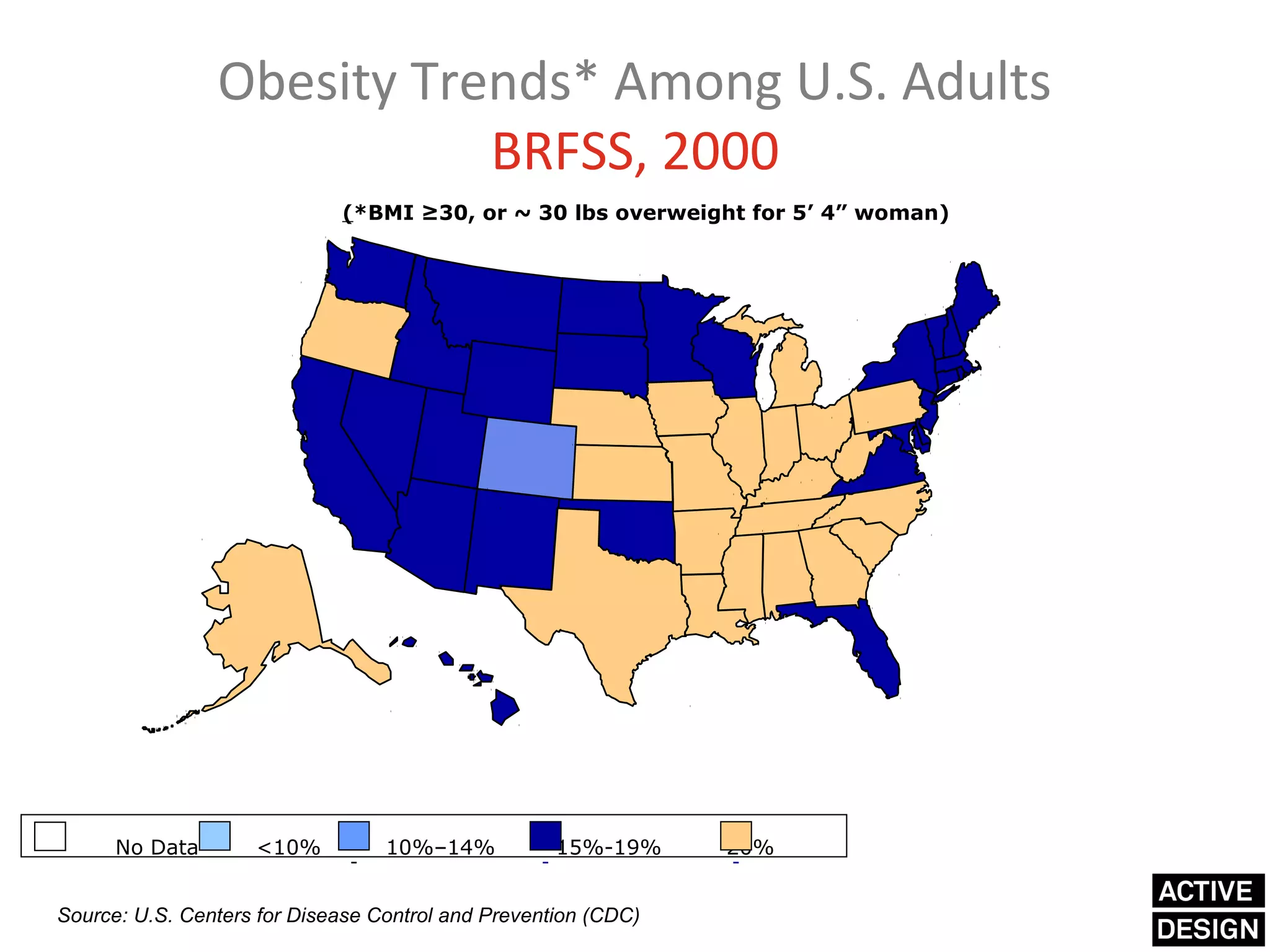
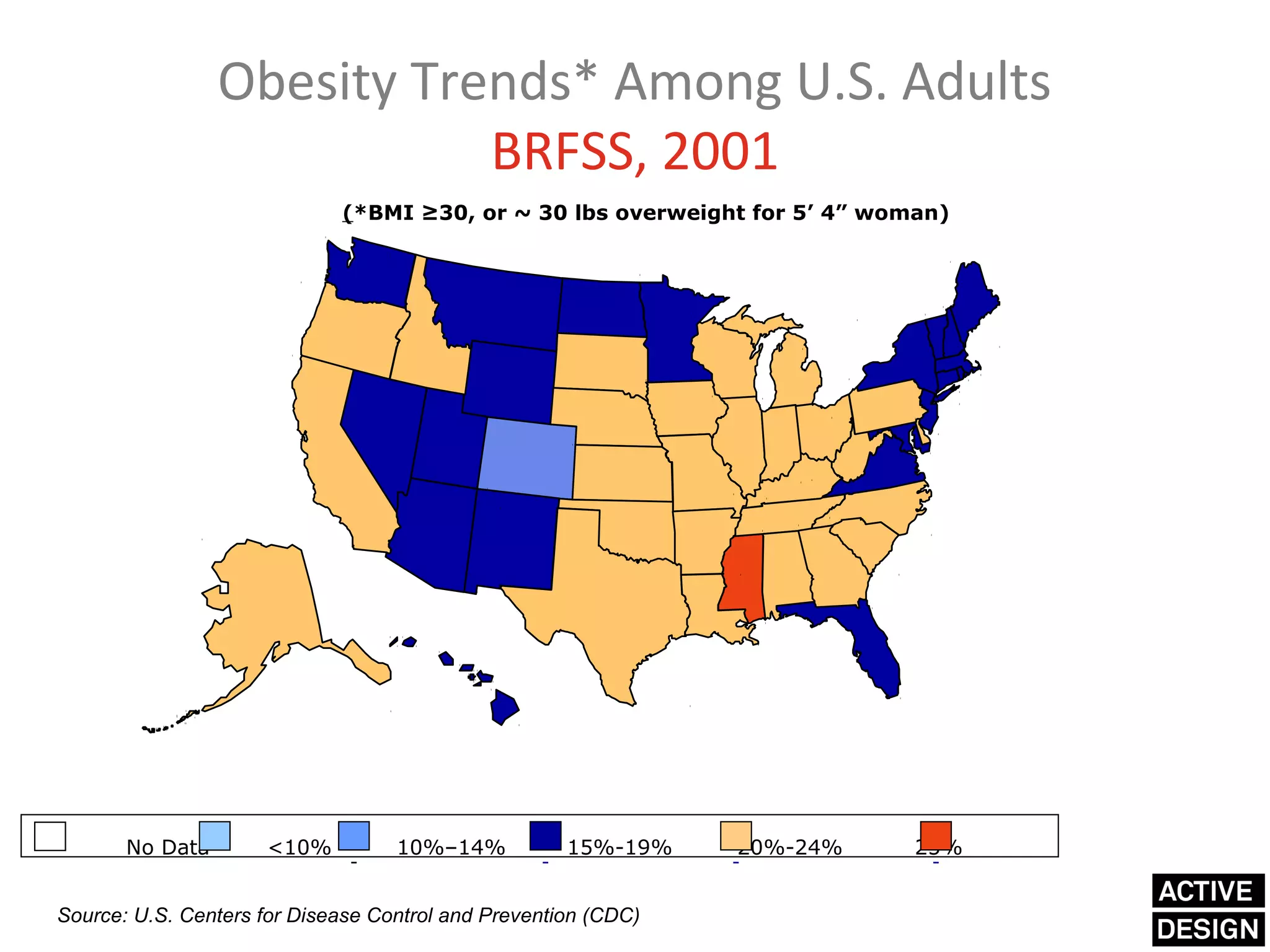
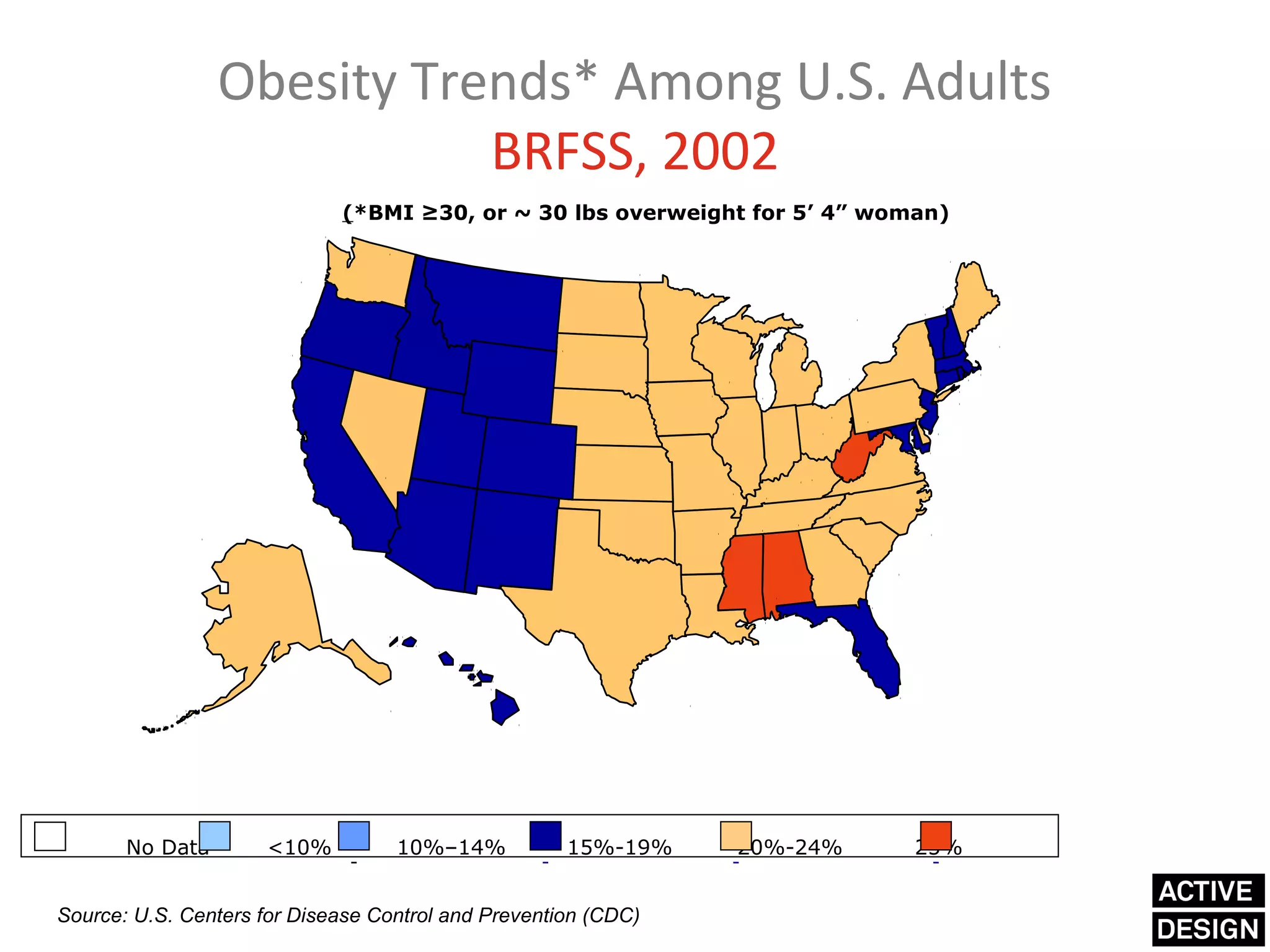
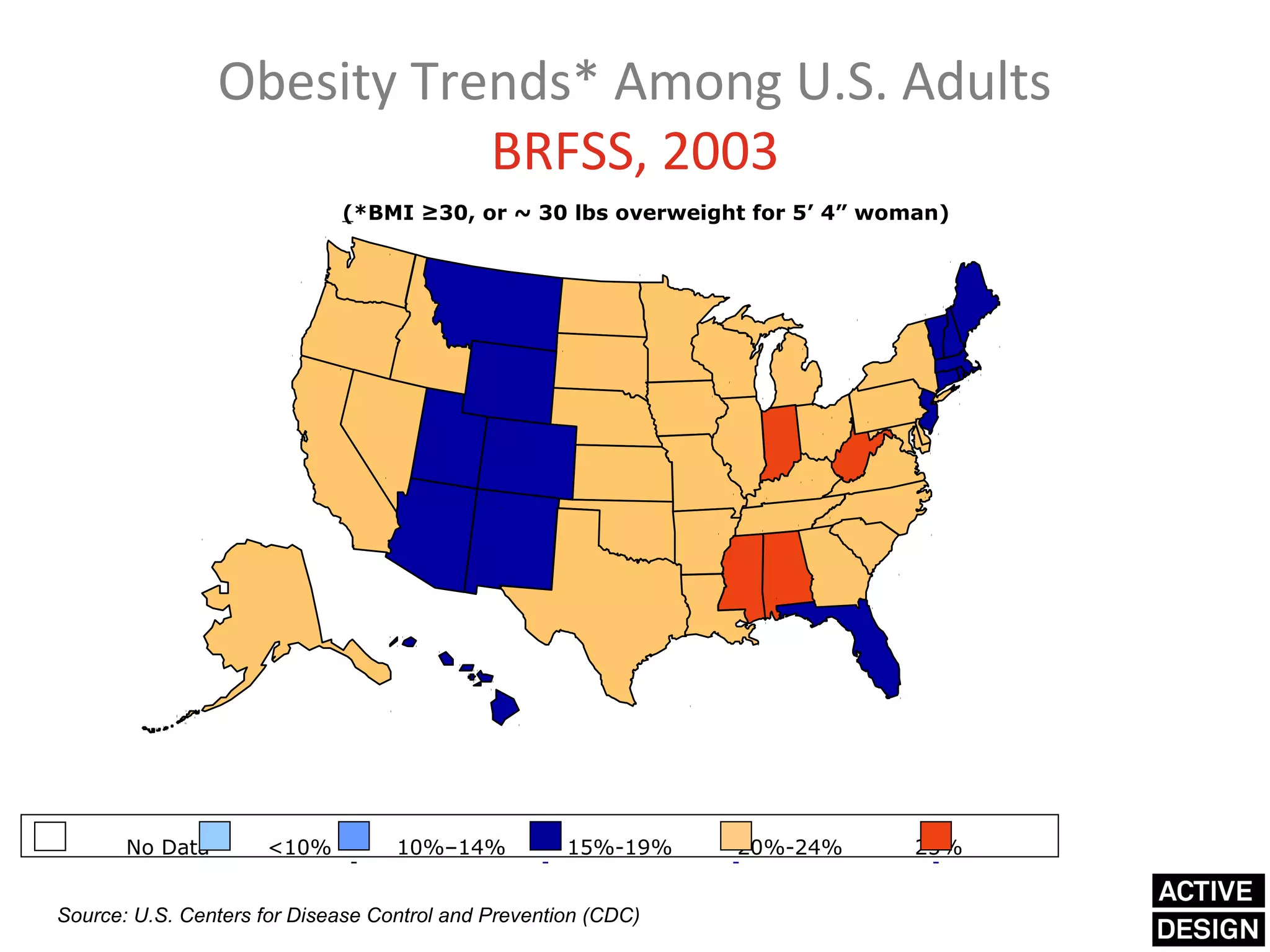
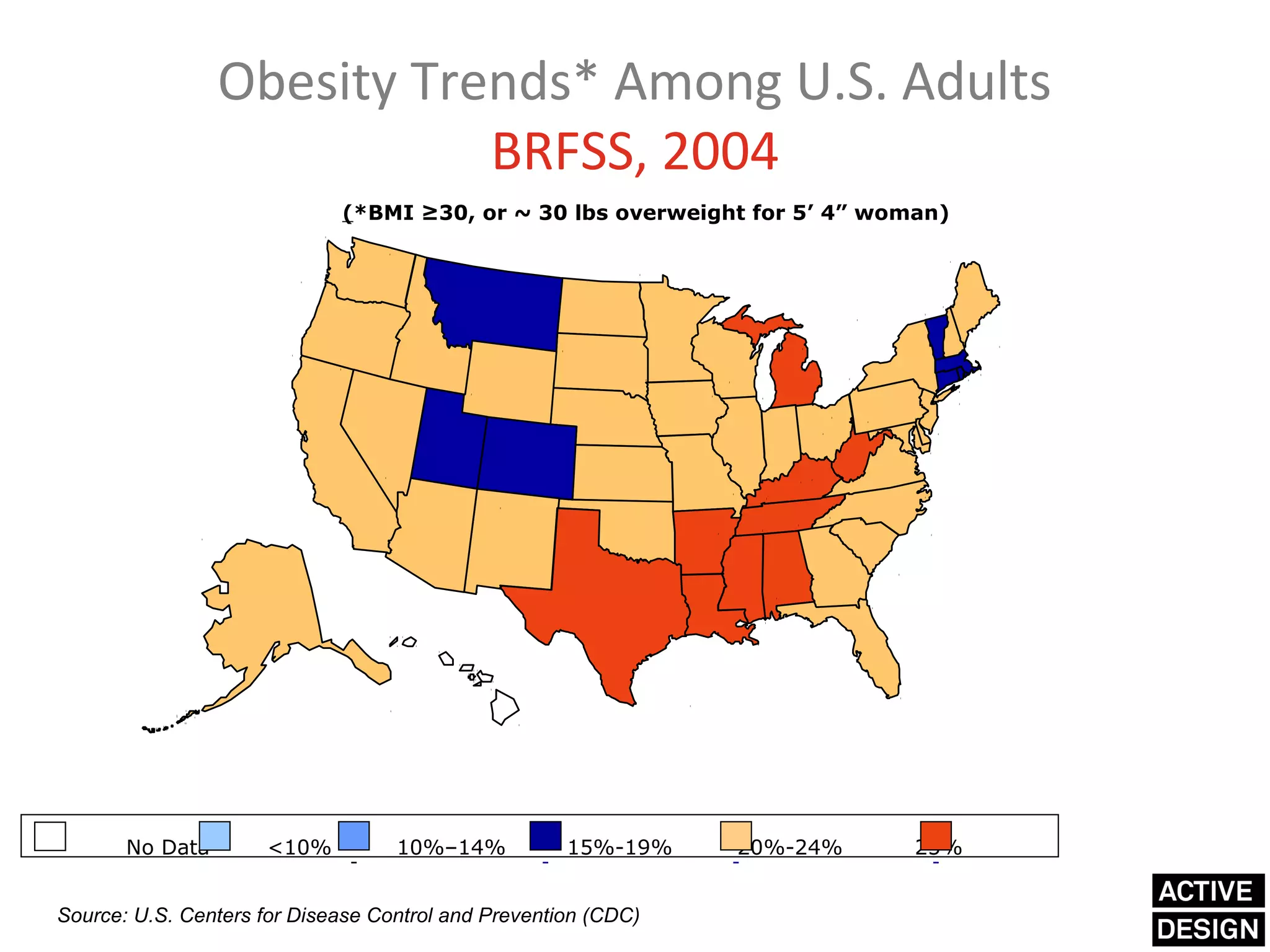
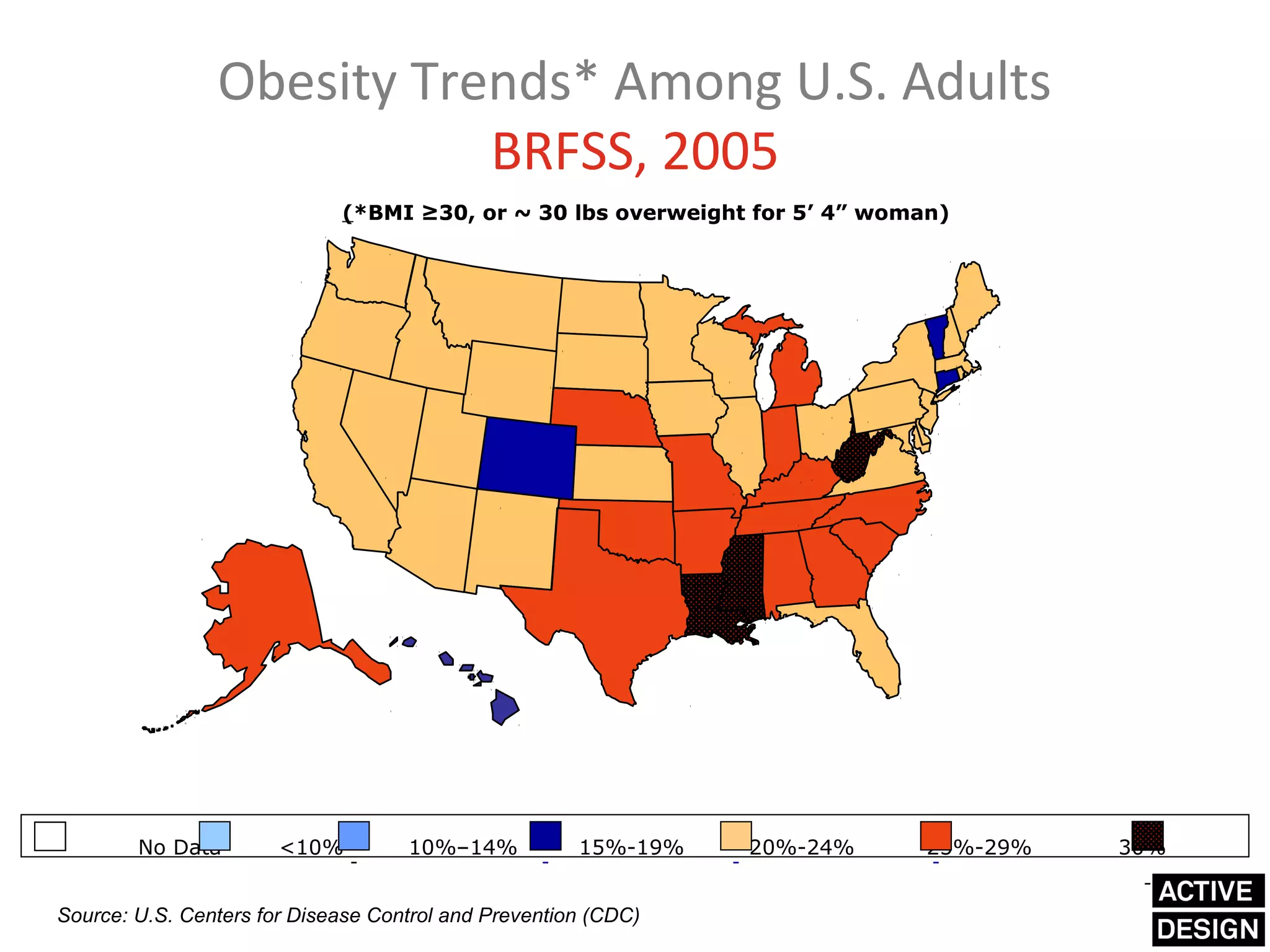
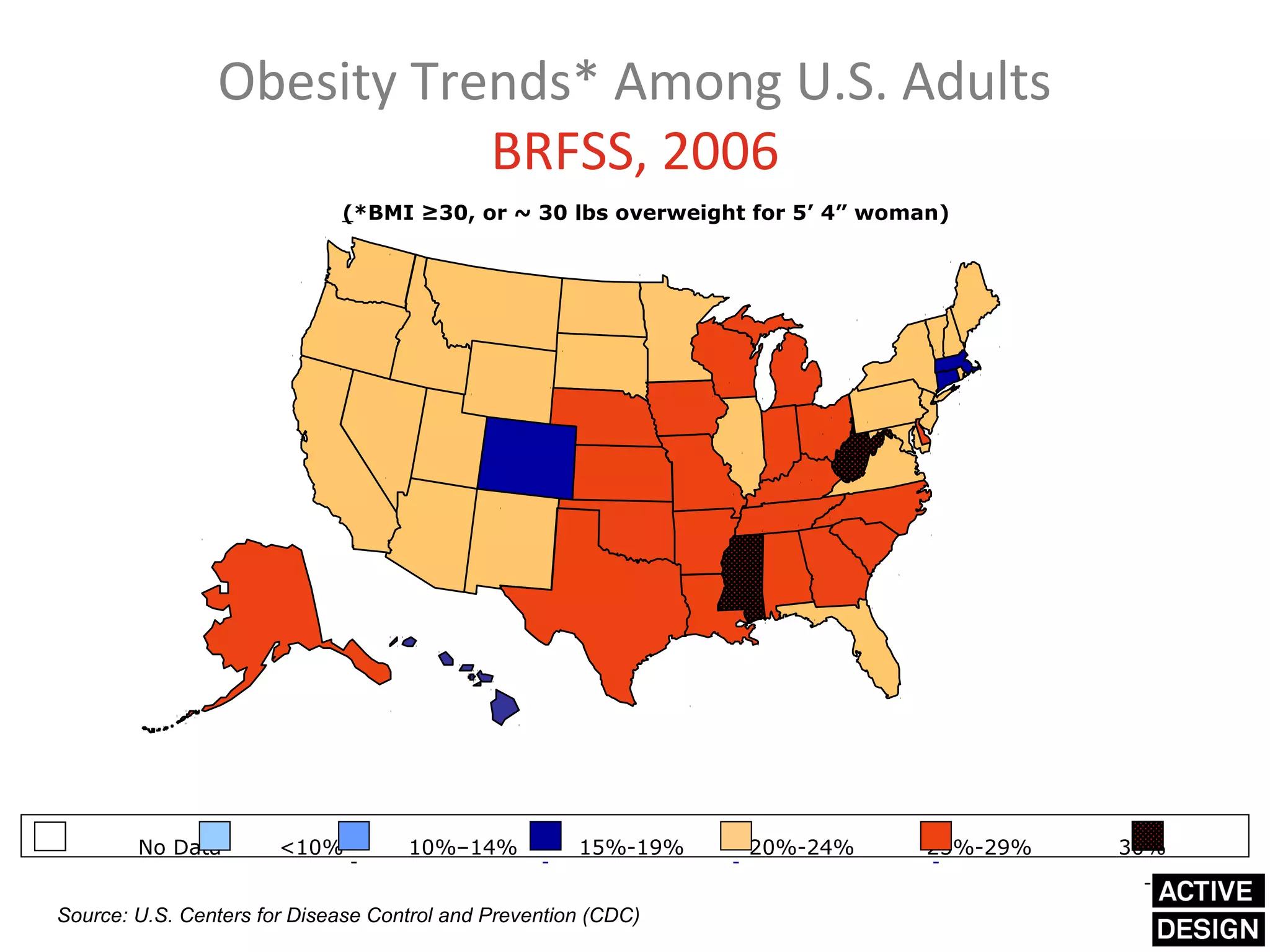
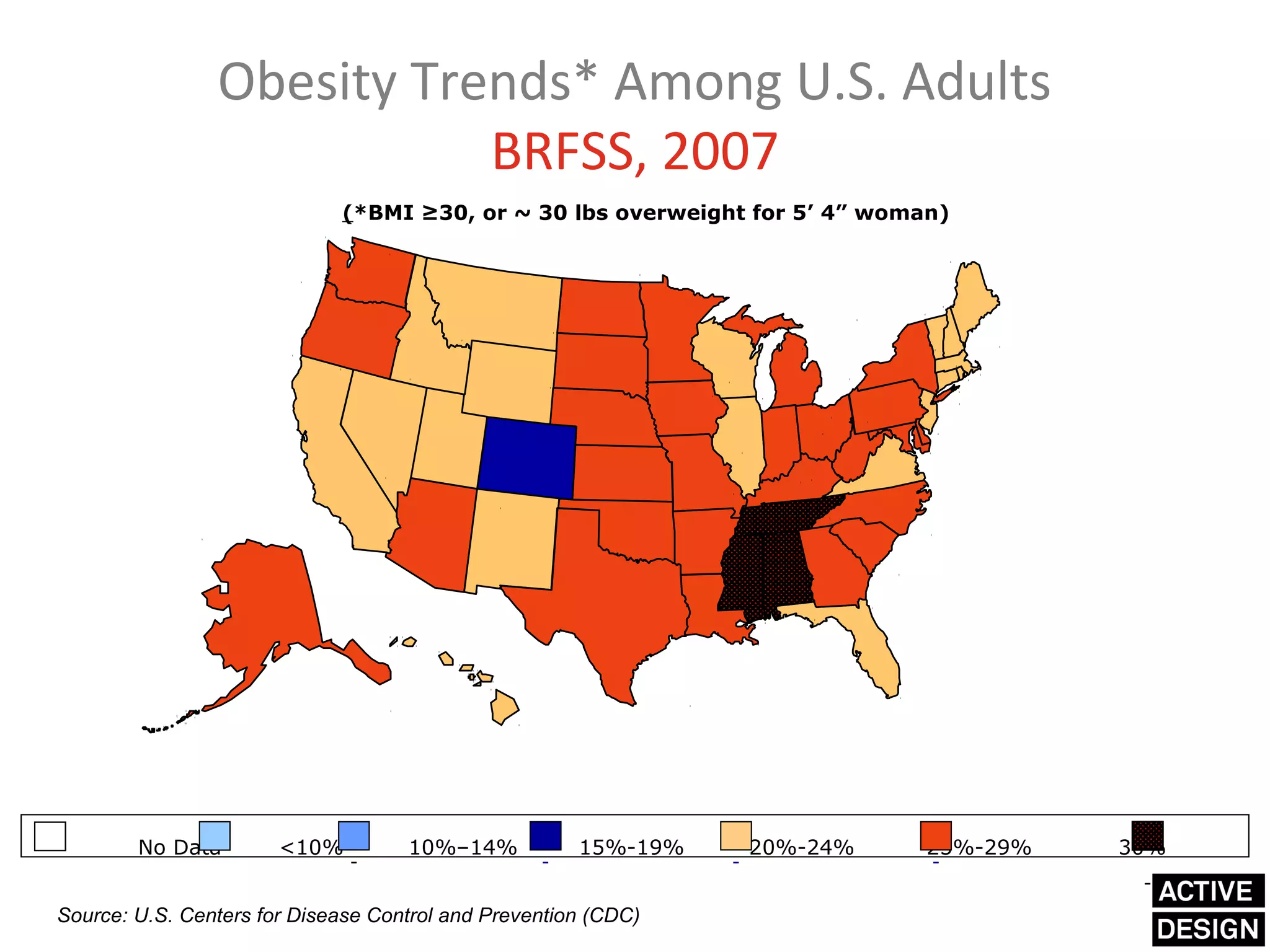
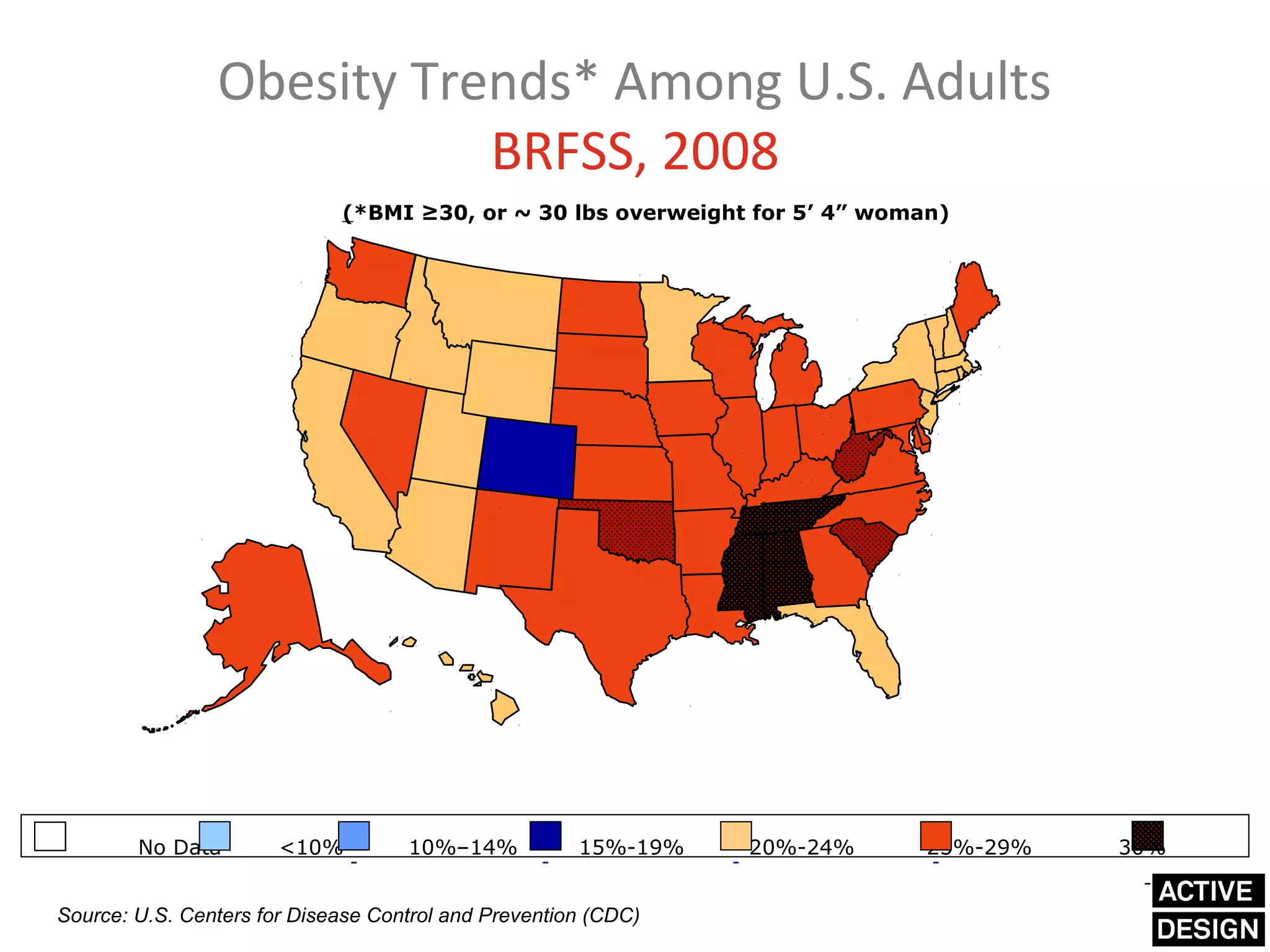
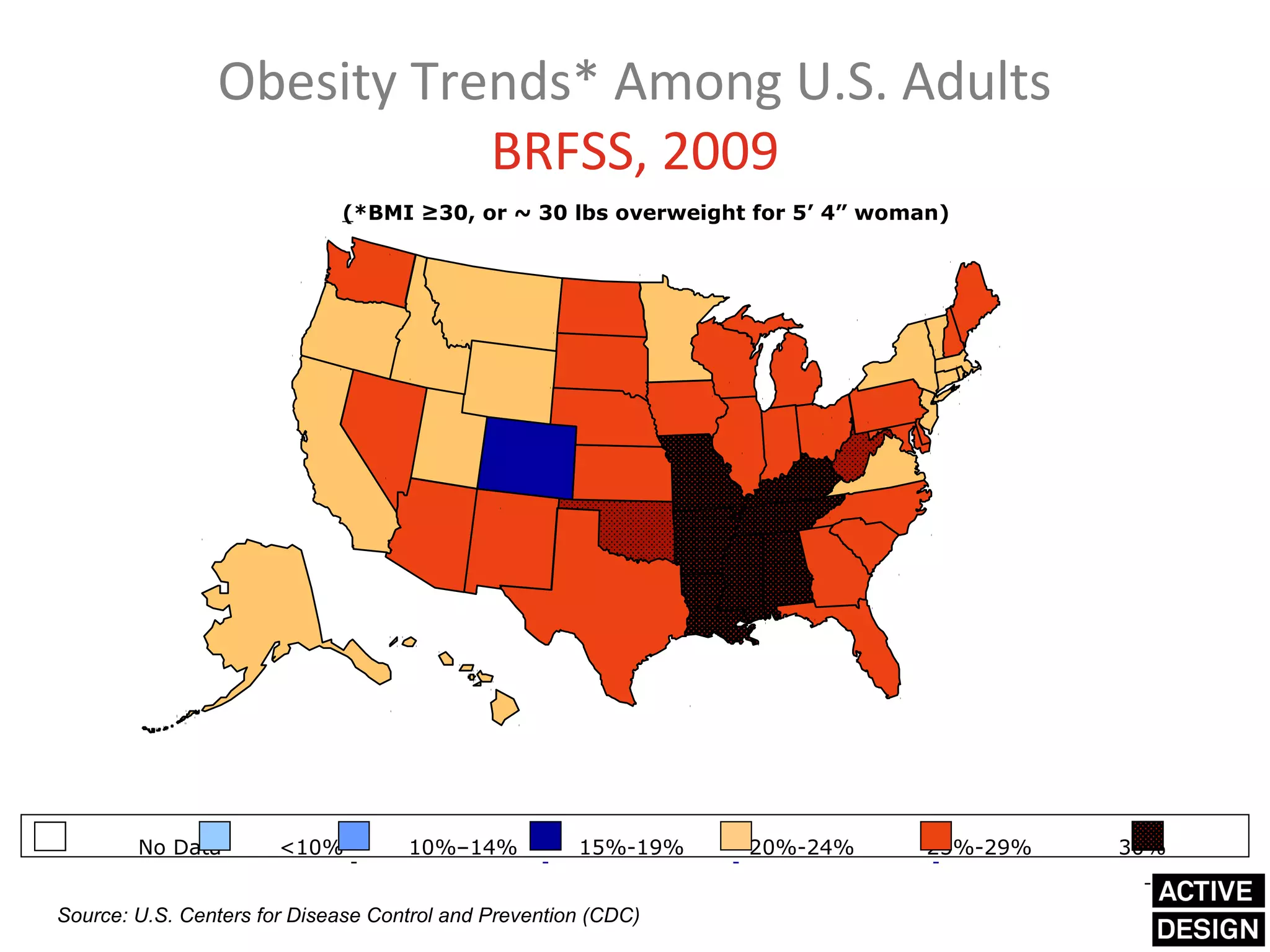
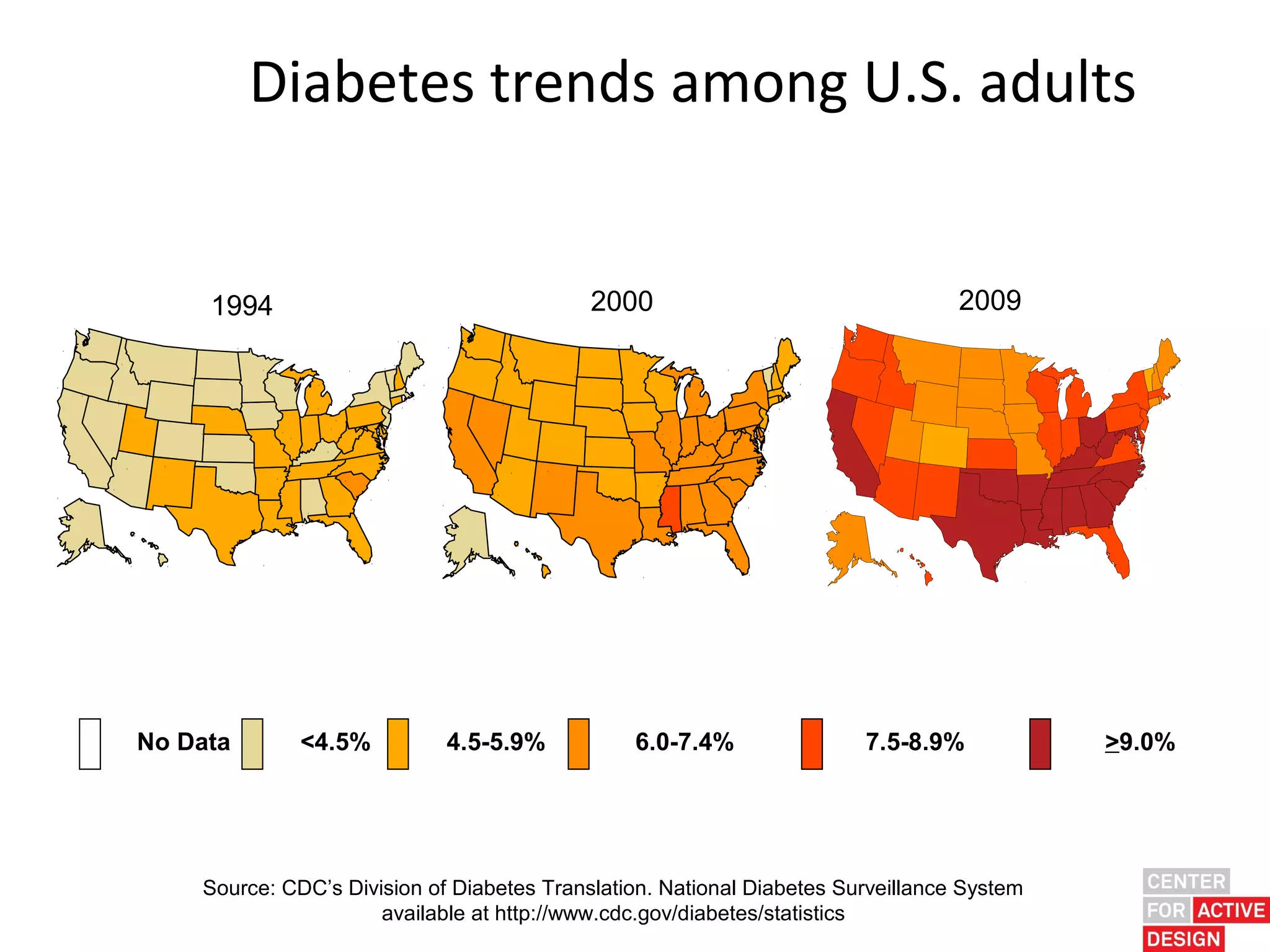
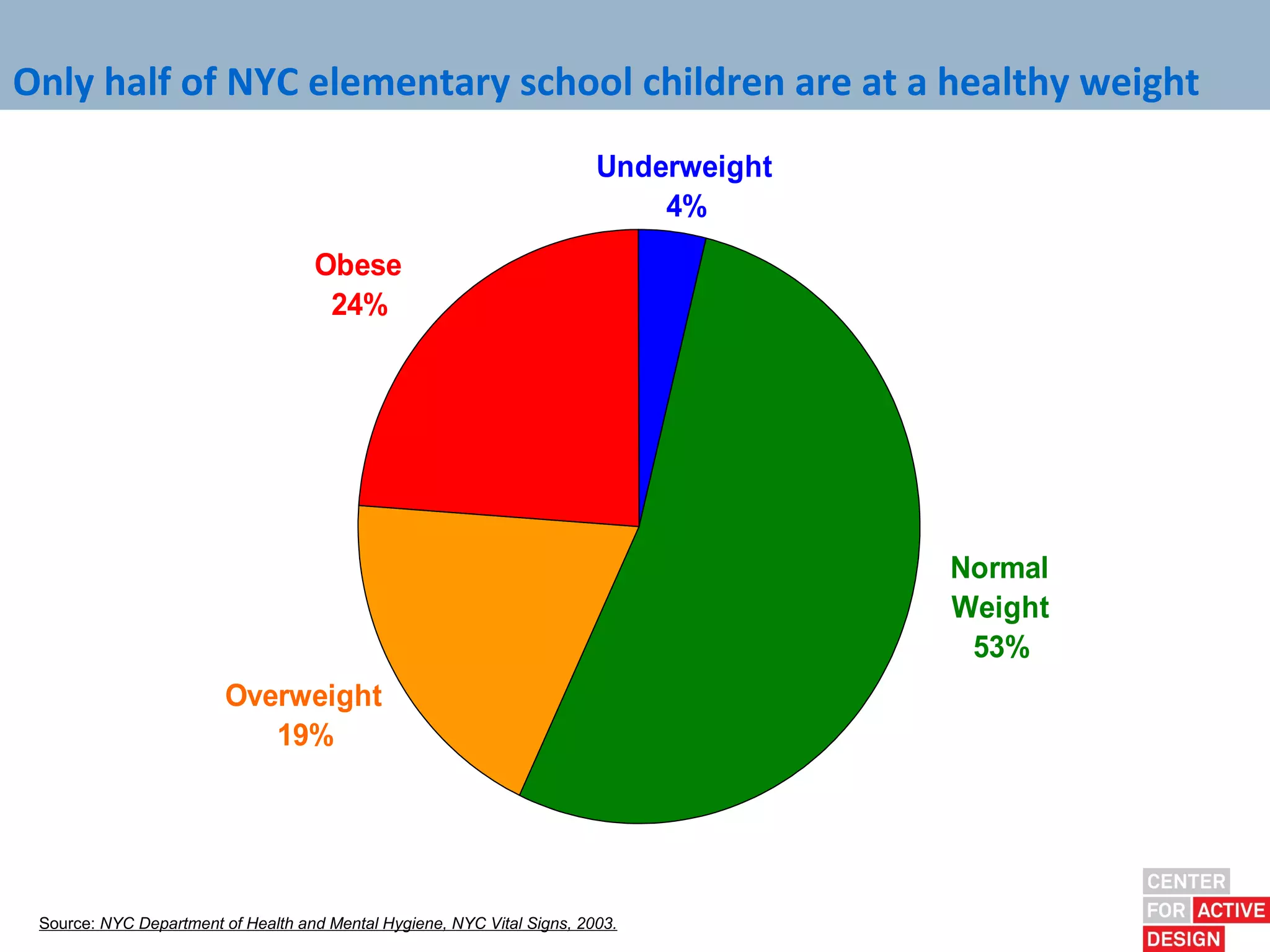
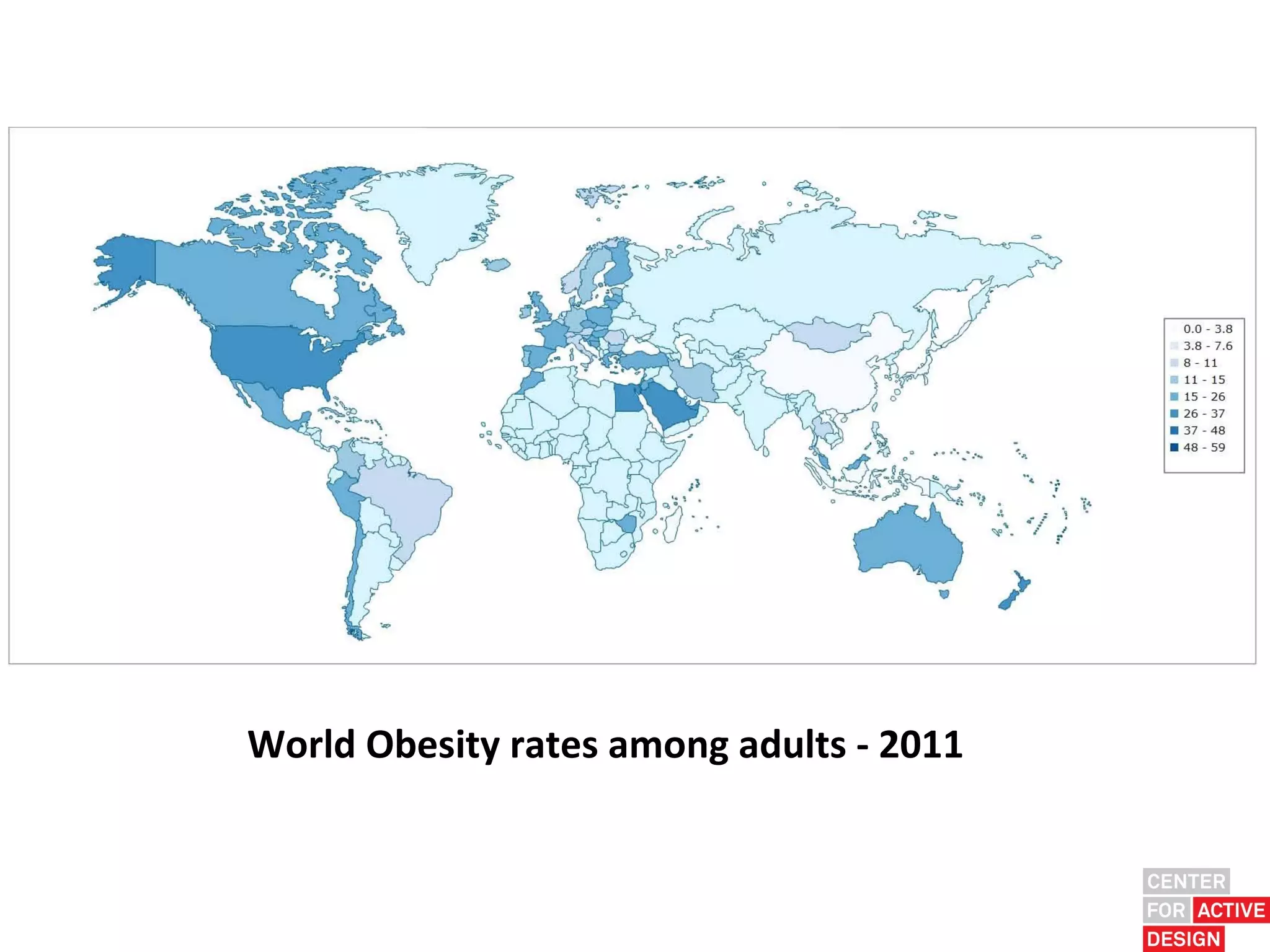

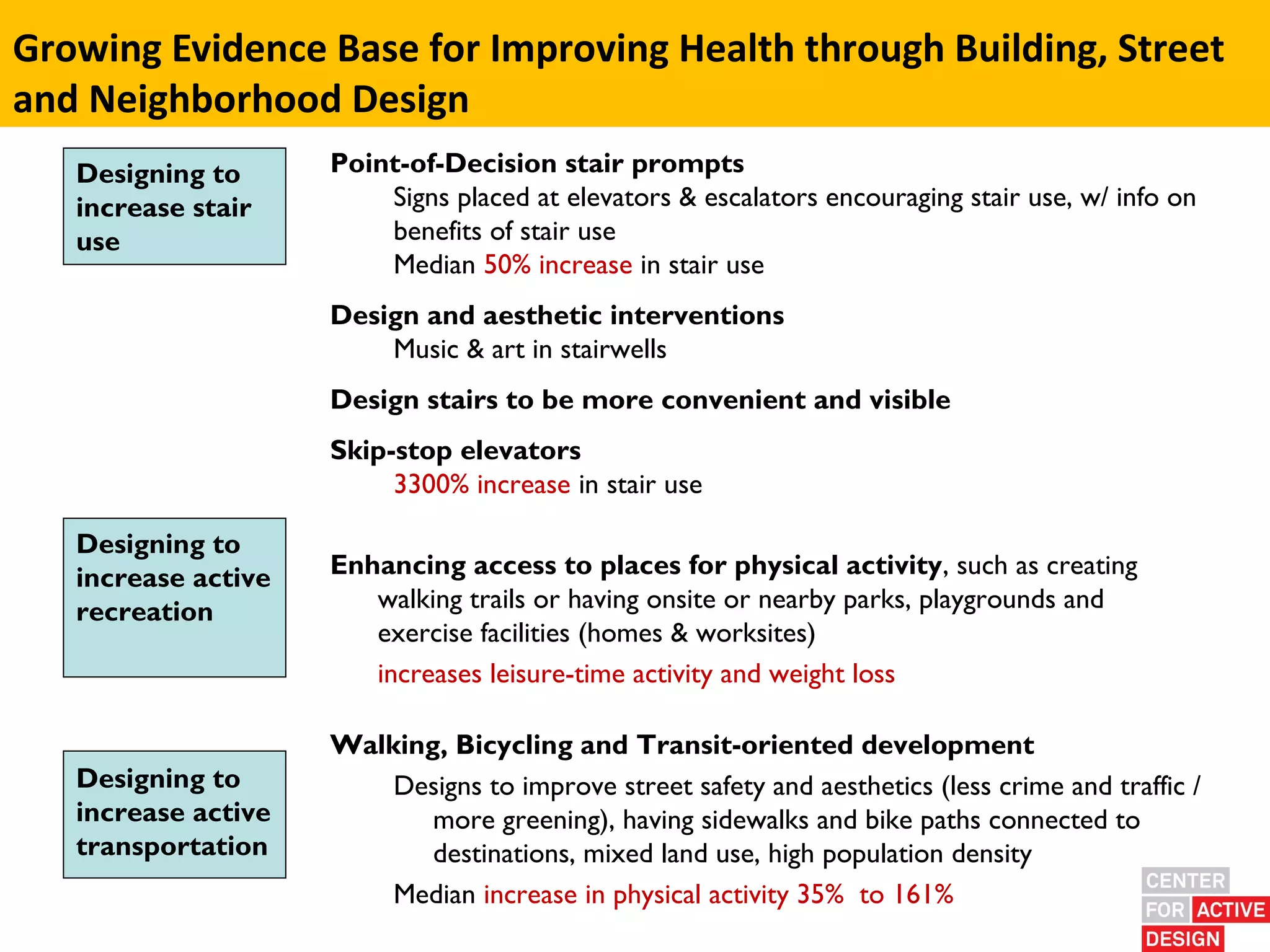
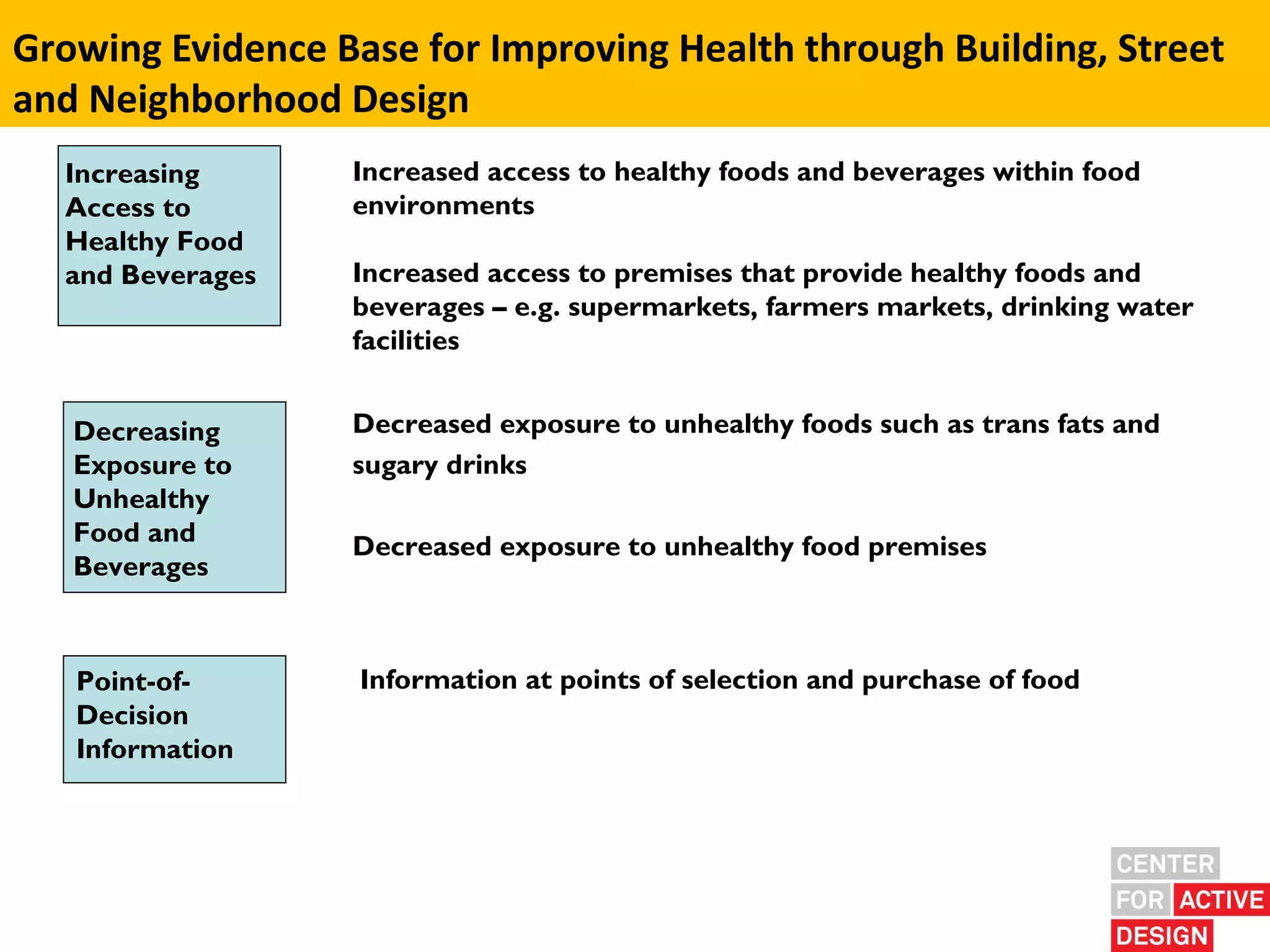
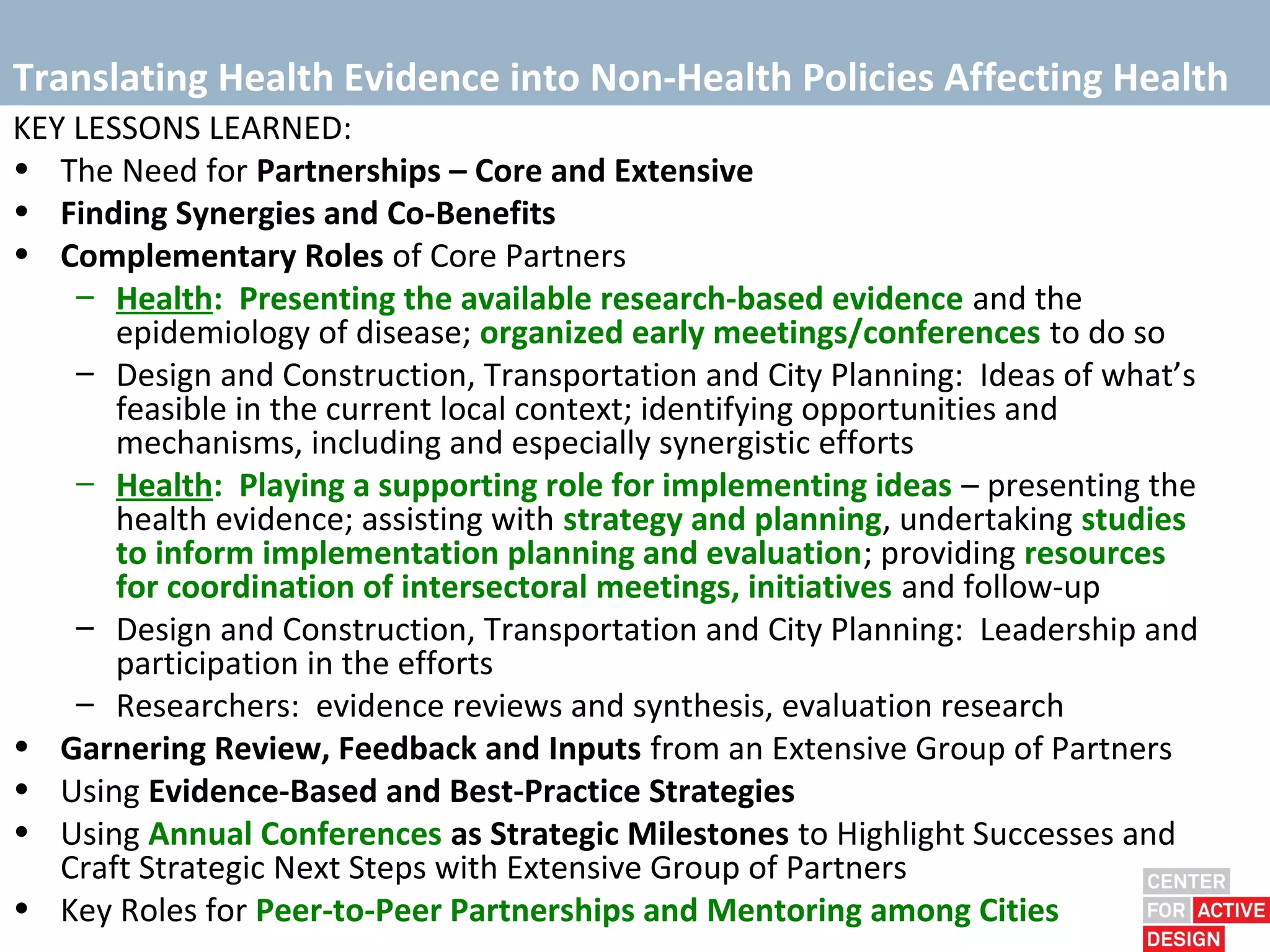

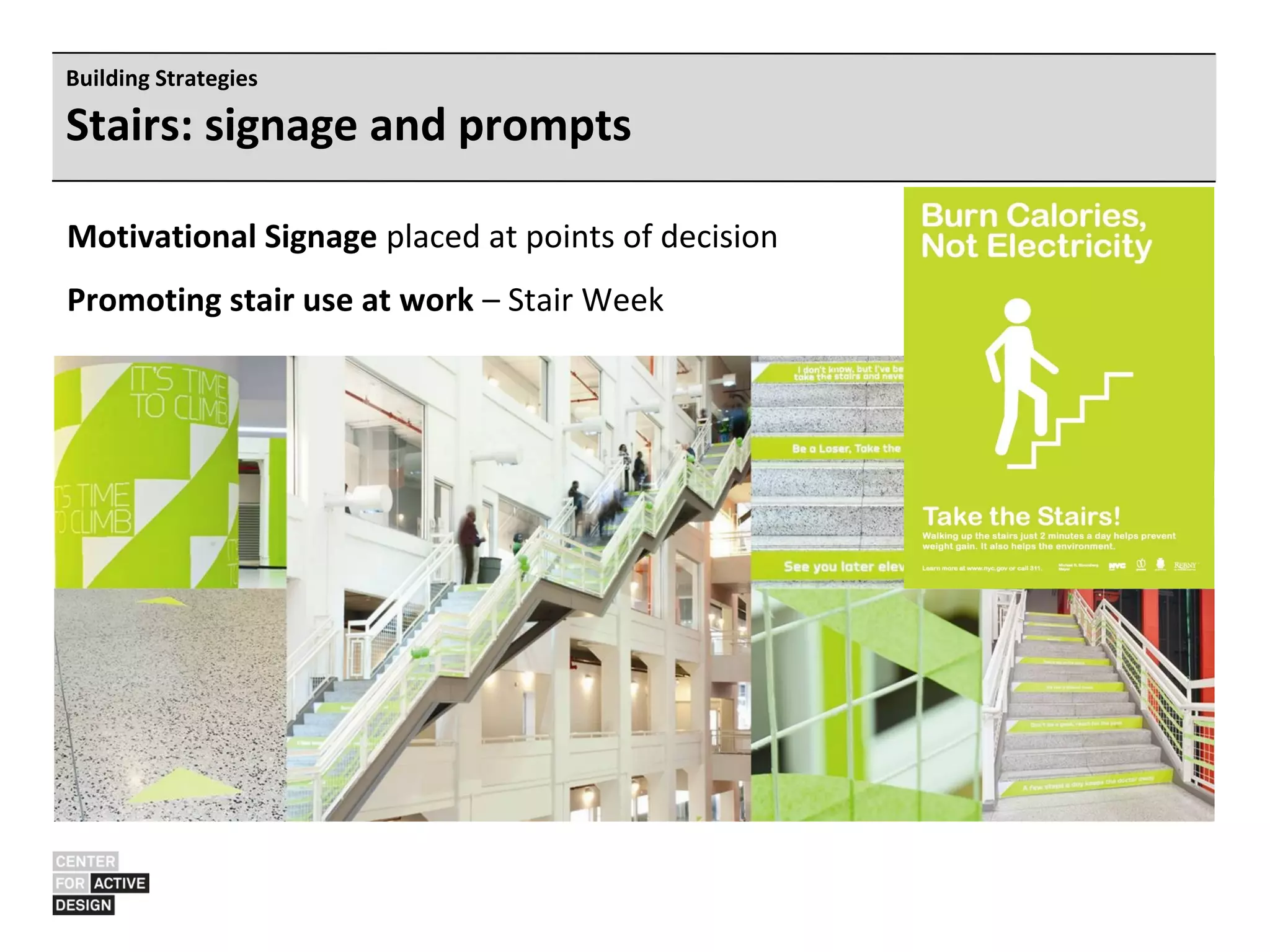
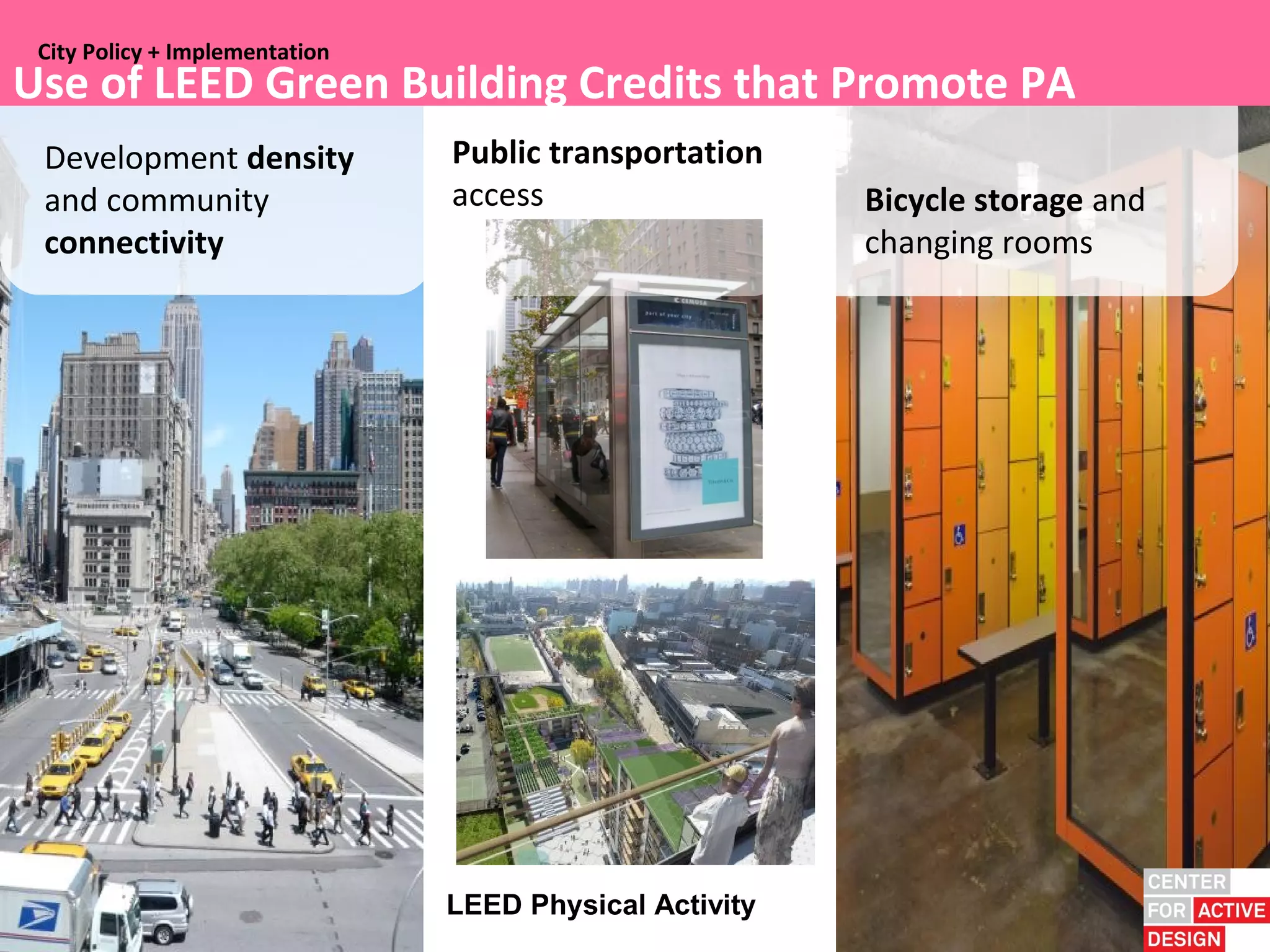
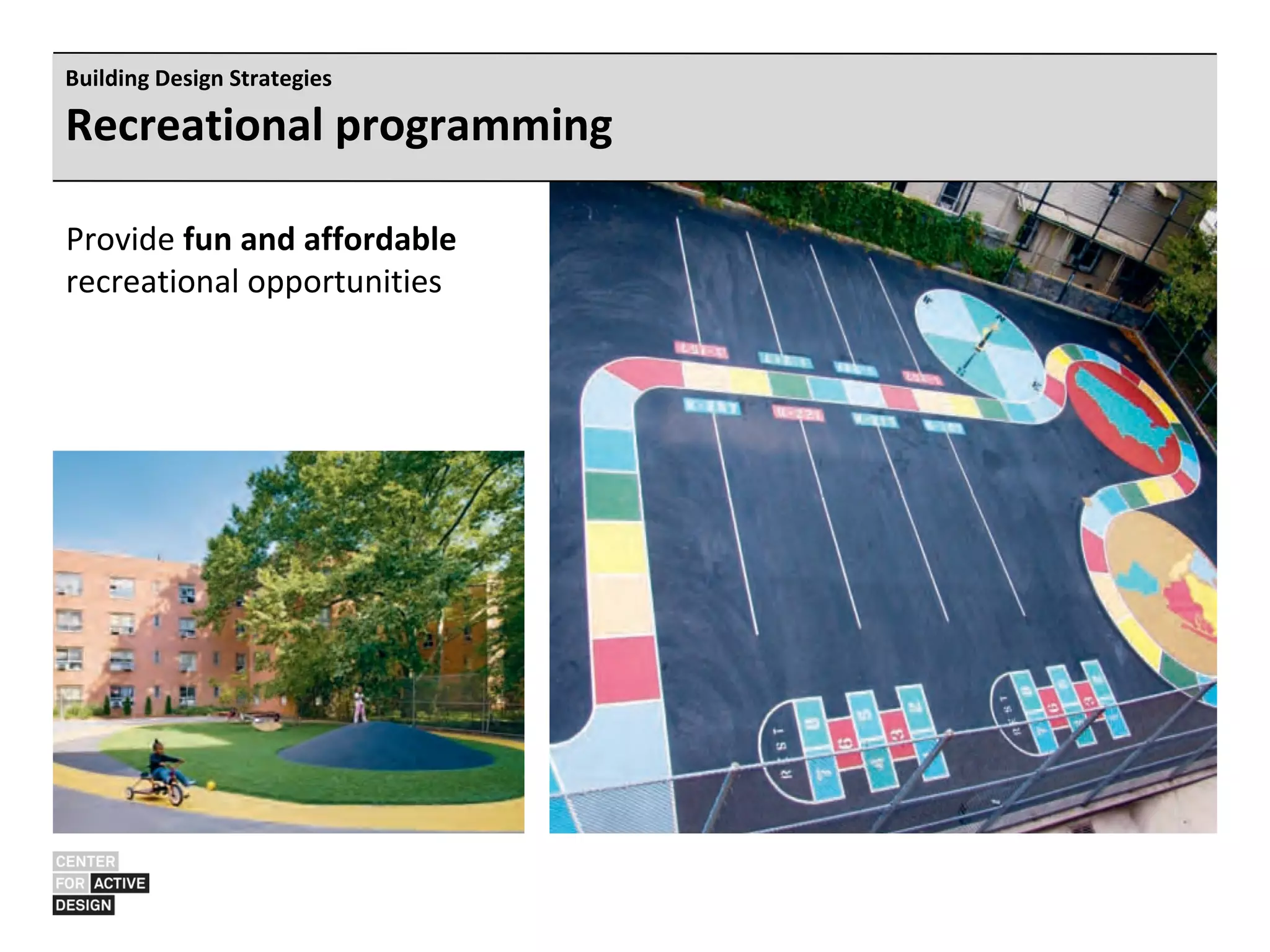
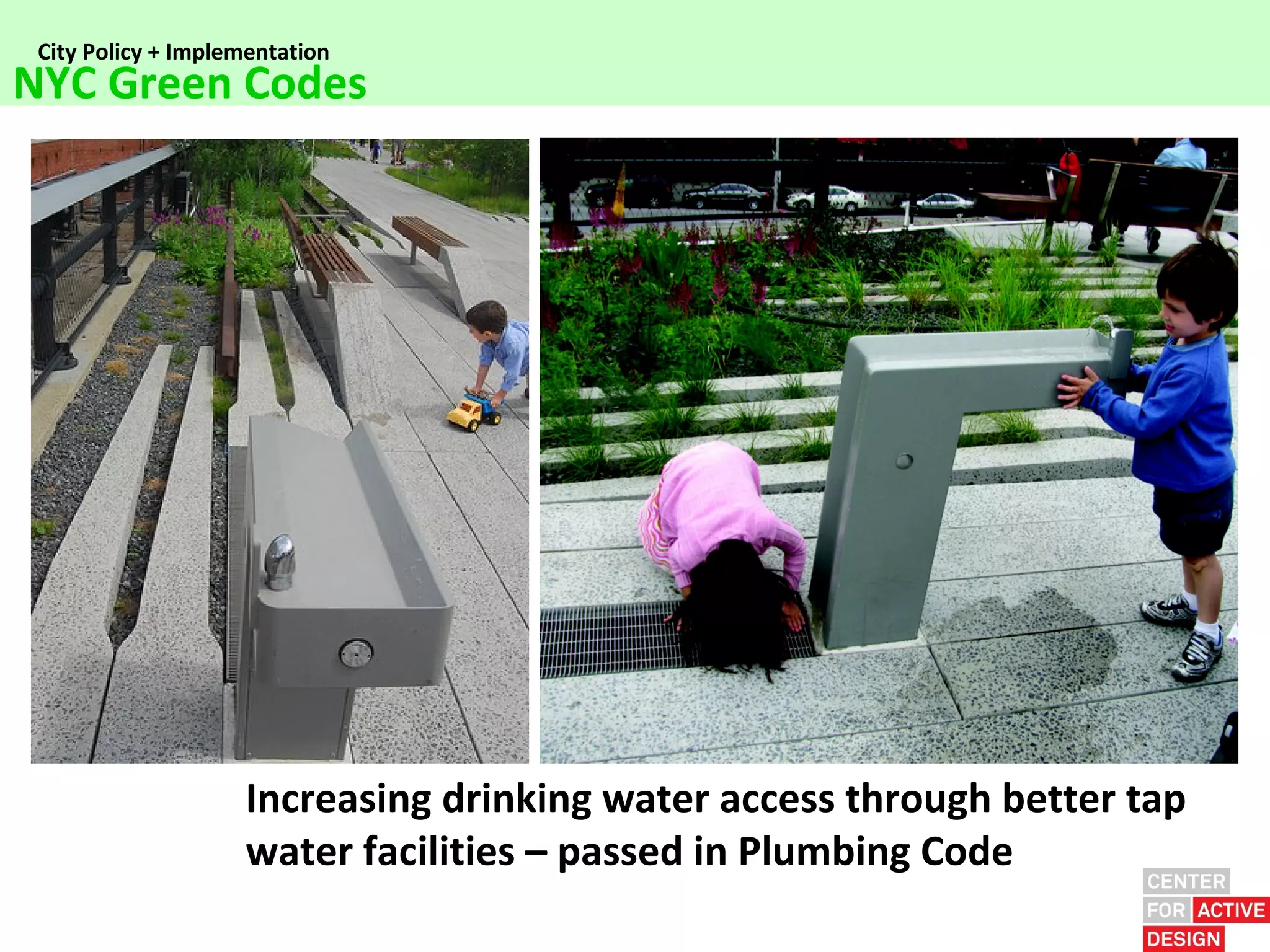







The document discusses the evolution of urban design and public health, highlighting the historical context of infectious diseases in 19th-century New York City and the emergence of chronic diseases today, such as obesity and diabetes. It emphasizes the importance of active design principles in creating environments that encourage physical activity, citing strategies like improving stair accessibility and enhancing neighborhood design. The document also outlines a collaborative framework among health, urban planning, and design professionals to implement effective interventions that promote healthier lifestyles.



































































