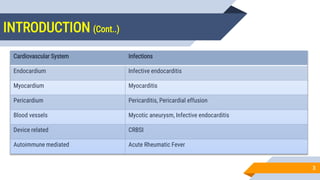
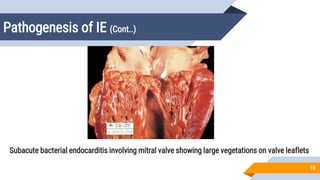
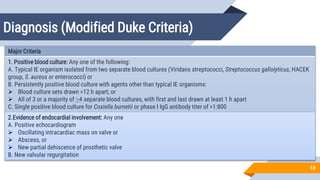
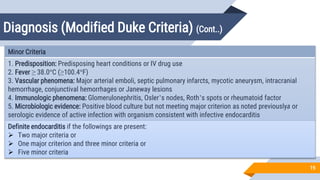
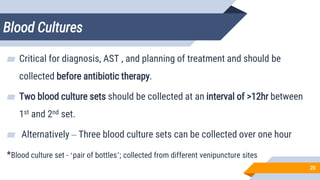
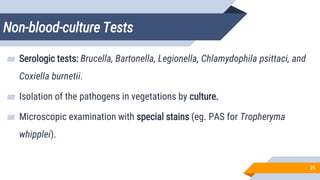
Cardiovascular system infections include infections of the heart and blood vessels, such as infective endocarditis, myocarditis, pericarditis, mycotic aneurysms, and device-related infections. Infective endocarditis refers to microbial invasion of heart valves or inner lining of the heart, which can result in the formation of vegetations. It is commonly caused by Staphylococcus aureus, viridans streptococci, enterococci, and other bacteria and fungi. Diagnosis involves blood cultures, echocardiography, and application of the Modified Duke Criteria. Treatment involves prolonged courses of antibiotics depending on the causative organism.