
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Blood stream infections1
Similar to Blood stream infections1 (20)
Recently uploaded
Recently uploaded (20)
Blood stream infections1
- 1. Bloodstream Infections Dr Neeta Khokhar Assist. Professor Microbiology Dept GMERS Medical College Gandhinagar
- 2. Learning objectives At the end of the session, the students will be able to understand: ▰ Etiological Agents of BSI ▰ Types of Bloodstream Infections ▰ Clinical Manifestations and laboratory Diagnosis ▰ Fever of Unknown Origin (FUO) 2
- 3. INTRODUCTION ▰ Blood stream infections (BSI) - presence of microorganisms in blood - constitute one of the most serious situations among infectious diseases. ▰ Microbial invasion of blood stream can have serious immediate consequences such as shock, multiple organ failure, and DIC (disseminated intravascular coagulopathies) 3
- 4. Terminologies ▰ Bacteremia - presence of bacteria in blood without any multiplication. ▰ Septicemia - bacteria circulate and actively multiply in the bloodstream and may produce their products (e.g. toxins) that cause harm to the host. ▰ Presence of viruses, parasites and fungi in blood - 'viremia', 'parasitemia' and 'fungemia' respectively 4
- 5. Types of Bacteremia 1. Transient bacteremia: ▰ Occur spontaneously or with minor events (brushing teeth or chewing food, instrumentation of contaminated mucosal site and surgery involving non- sterile site) ▰ May also lead to septicemia 5
- 6. Types of Bacteremia (Cont..) 2. Continuous bacteremia: ▰ Organisms are released into the bloodstream at a fairly constant rate. ▰ Septic shock, endocarditis and other endovascular infections. 6
- 7. Types of Bacteremia (Cont..) 3. Intermittent bacteremia: bacteria are released into blood intermittently ▰ Undrained abscess (bacteria are released approximately 45 minutes before a febrile episode). ▰ Early course of meningitis, pneumonia, pyogenic arthritis and osteomyelitis. 7
- 9. ETIOLOGICAL AGENTS OF BSI Pathogens of all four major groups of microbes— ▰ Bacteria ▰ Viruses ▰ Fungi ▰ Parasites 9
- 10. Bacterial Etiology ▰ Bacterial agents account for the majority of bloodstream infections. ▰ Common agents causing primary BSI- typhoidal salmonellae, brucellae or spirochetes (Leptospira, Borrelia), HACEK group of pathogens, viridans streptococci and rickettsiae (infect vascular endothelium). 10
- 11. Bacterial Etiology (Cont..) ▰ Primarily infect other sites and subsequently spill over to the blood stream to cause secondary BSI: Gram-positive cocci: Staphylococci, beta hemolytic streptococci, enterococci and pneumococci), Gram-negative cocci: meningococci Gram-positive bacilli : Bacillus anthracis and Listeria 11
- 12. Bacterial Etiology (Cont..) ▰ Gram-negative bacilli: E. coli, Klebsiella, Enterobacter, non-fermenters (e.g. Pseudomonas, Acinetobacter, Burkholderia, Stenotrophomonas) Haemophilus, Aeromonas, etc. ▰ Anaerobes: Bacteroides 12
- 13. Viral Etiology ▰ HIV & other human retroviruses–attack CD4 T lymphocytes and macrophages. ▰ Agents of hemorrhagic fever - dengue, chikungunya, Ebola, Marburg, Lassa, yellow fever, and other viruses – they infect endothelial cells (Yellow fever virus) 13
- 14. Viral Etiology (Cont..) ▰ Epstein-Barr virus- Invades lymphocytes - causes infectious mononucleosis and various malignancies. ▰ Cytomegalovirus- Invades monocytes, polymorphonuclear cells, and lymphocytes - causes hepatitis and congenital infections. 14
- 15. Parasitic Etiology ▰ Parasites that directly infect RBCs- Plasmodium and Babesia ▰ Parasites that may be found in the blood stream before they migrate to other tissues or organs; e.g. include tachyzoites of T.gondii, amastigote forms of Leishmania, and trypomastigote forms of Trypanosoma. ▰ Parasites that may be present in lymphatics and come to bloodstream transiently; e.g. microfilariae of filarial parasites. 15
- 16. Fungal Etiology ▰ Fungemia - occur primarily in immunocompromised patients ▰ Candida species – MC agent; (8-10% of all nosocomial BSI) C.albicans & non-albicans Candida species - C. tropicalis, C. parapsilosis & C. auris ▰ Agents of systemic mycoses (Histoplasma, Blastomyces, Coccidioides, and Paracoccidioides). 16
- 18. TYPES OF BLOODSTREAM INFECTIONS ▰ There are two major categories of bloodstream infections (BSIs): Intravascular Extravascular. 18
- 19. Factors contributing to initiation of BSI ▰ Immunosuppression ▰ Use of broad-spectrum antimicrobial agents ▰ Invasive procedures ▰ Extensive surgeries that allow the bacteria to access the blood ▰ Prolonged survival of debilitated patients 19
- 20. Intravascular Bloodstream Infections ▰ They originate within the cardiovascular system which includes: Infection of the heart (endocarditis, myocarditis and pericarditis) Infection of blood vessels 20
- 21. Extravascular Bloodstream Infections ▰ Organisms multiply at the primary site such as lungs and are drained by lymphatics and reach the bloodstream. ▰ The organisms are either removed by the cells of the reticuloendothelial system or they multiply more widely and thereby causing septicemia. 21
- 22. Extravascular Bloodstream Infections (Cont..) ▰ Portal of entry: Most common portals of entry - genitourinary tract (25%), Followed by respiratory tract (20%), abscesses (10%), surgical site wound infections (5%), and biliary tract (5%). In up to 25% of cases, the portal of entry remains uncertain 22
- 23. Bacteria causing extravascular bloodstream infections (BSIs) and their common sources 23 Bacteria Portal of entry/sources E. coli and other gram-negative bacteria such as Klebsiella, Proteus, Enterobacter, Pseudomonas Urinary tract (most common), Intestine (rarely) Haemophilus influenza type b Meninges, epiglottis, lungs Pneumococcus Meninges, lungs Brucella Reticuloendothelial system Salmonella Typhi Small intestine, lymph nodes and reticuloendothelial system Listeria Intestine, meninges Staphylococcus aureus and coagulase negative staphylococci Surgical site infections
- 25. CLINICAL MANIFESTATIONS ▰ BSI - have a bacteremia stage followed by a septicemic stage. ▰ Clinical manifestations are evident only in the septicemic stage - bacteria multiply and release their products (e.g. toxins) which travel to various organs affecting their functions. ▰ Based on the severity and the extent of organ failure – 2 stages of BSI: sepsis and septic shock 25
- 26. Definition of sepsis and the assessment of severity and organ failure 26 Sepsis Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection SOFA score Sepsis is diagnosed by SOFA (Sepsis-related organ failureassessment) score which in turn depends on six parameters. 1. Respiratory system—PaO2/FiO2 2. Coagulation system—Platelet count 3. Liver—Serum bilirubin 4. Cardiovascular—Mean arterial pressure (MAP) 5. Central nervous system—Glasgow coma scale score 6. Renal—Serum creatinine and urine output Organ dysfunction can be identified as an acute change in the total SOFA score ≥2 points following the infection
- 27. Definition of sepsis and the assessment of severity and organ failure (Cont..) 27 qSOFA (Quick SOFA) Criteria Determination of SOFA score takes considerable time as it depends upon a number of laboratory parameters. However, before the result of SOFA score is available, sepsis can promptly be identified at the bedside with qSOFA score Respiratory rate ≥22/min Altered mentation Systolic blood pressure ≤100 mm Hg Septic shock It is a subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound Patients with septic shock can be identified with a clinical construct of sepsis with: Persisting hypotension requiring vasopressors to maintain MAP (mean arterial pressure) ≥65 mm Hg and Serum lactate level >2 mmol/L (18 mg/dL) despite adequate volume resuscitation Patients with septic shock have a mortality of >40% in contrast to 10%, for sepsis cases
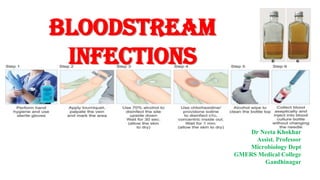
- 29. Specimen Collection for Blood Culture ▰ Site: Blood for culture should always be collected in pairs; from two separate venipuncture and 2 separate skin decontamination process. ▰ Preparation of the site: To avoid contamination with skin flora, blood should be collected under strict aseptic conditions using sterile disposable syringe. ▰ Skin decontamination ▰ Timing of collection: Blood - collected before starting antimicrobial 29
- 30. Specimen Collection for Blood Culture (Cont..) ▰ Blood volume: At least 8–10 mL of blood per bottle for an adult and 1–3 mL per pediatric bottle is recommended. ▰ Number of blood cultures: At least 2–3 blood culture sets (each set consists of two bottles: 1 aerobic and 1 anaerobic) are required. ▰ Dispensing: Collected blood is then directly dispensed into either blood culture bottle at the bedside (conventional or automated blood culture). 30
- 31. Specimen Collection for Blood Culture (Cont..) ▰ Transport of blood specimen: The collected blood is gently mixed with the broth and then transported immediately to the Microbiology laboratory. ▰ In case of delay, blood culture bottle should never be refrigerated. ▰ It can be kept at 350C in an incubator (if available) or left at room temperature. 31
- 32. Steps of collection of blood for culture 32
- 33. Conventional Culture Medium Types of media: ▰ A. Monophasic medium:50–100 mL of brain heart infusion (BHI) broth. ▰ B. Castaneda’s biphasic medium: BHI agar slope and BHI broth 33
- 34. Conventional Culture Medium (Cont..) ▰ Dilution: The blood is inoculated in the medium at a dilution of 1:5 so that the antibacterial components in the blood, if any, will get diluted. ▰ SPS (sodium polyanethol sulfonate) is added to the medium as an anticoagulant. It also counteracts the bactericidal action of blood. ▰ Incubation: Upon receipt, the bottles should be directly incubated in the upright position at 37° C for up to 7 days. 34
- 35. Conventional Culture Medium (Cont..) ▰ Repeat subcultures are made from the BHI broth onto blood agar and MacConkey agar. 35
- 36. Automated Culture Media ▰ BACTEC and BacT/ALERT ▰ Bact/ALERT Virtuo- most advanced system ▰ Growth is continuously monitored, & reading is recorded every 15–20 min. 36
- 37. Automated Culture Media (Cont..) ▰ When the growth is detected, the system gives a positive signal. ▰ Then the bottle is removed and processed similarly as done for conventional bottles. 37
- 38. Identification ▰ The isolated organism is identified by colony morphology, Gram staining, followed by either conventional biochemical reactions or automated identification system such as MALDI -TOF or VITEK. 38
- 39. Antimicrobial Susceptibility Test ▰ AST is carried out for guiding the institution of appropriate therapy. ▰ MIC based method (e.g., VITEK) is preferred over disk diffusion ▰ It is ideal for endocarditis isolates, especially while reporting susceptibility of penicillin. 39
- 40. Treatment ▰ Due to higher prevalence of MDROs and higher mortality in sepsis, antibiotics should be instituted at the earliest, as soon as sepsis is clinically suspected. 40
- 41. Treatment (Cont..) ▰ De-escalation approach is usually followed: ▰ Empirical treatment consists of higher class of antimicrobials with both gram-negative and gram-positive coverage; e.g. carbapenem such as meropenem plus vancomycin. Definitive treatment can be tailored according to AST report. 41
- 42. FEVER OF UNKNOWN ORIGIN (FUO) 42
- 43. FEVER OF UNKNOWN ORIGIN (FUO) ▰ Reserved only for prolonged febrile illnesses without an established etiology despite of intensive evaluation and diagnostic testing. 43
- 44. Definitions ▰ Petersdorf and Beeson had defined FUO in 1961 as patients having: Temperatures of >38.3°C (>101°F) at least on two occasions; duration of more than 3 weeks Failure to reach a diagnosis despite 1 week of inpatient investigation 44
- 45. The current definition of FUO ▰ 1. Fever ≥38.3°C (≥101°F) on at least two occasions ▰ 2. Duration of illness of ≥3 weeks ▰ 3. No known immunocompromised state ▰ 4. Diagnosis that remains uncertain after a thorough history-taking, physical examination, and the following obligatory investigations: 45
- 46. The current definition of FUO (Cont..) ▰ 4. Diagnosis that remains uncertain after a thorough history-taking, physical examination, and the following obligatory investigations: ESR and CRP (C-reactive protein) level Platelet count, leukocyte count (total and differential), and hemoglobin Electrolytes, creatinine, total protein, ferritin and protein electrophoresis Enzymes - alkaline phosphatase, alanine aminotransferase, aspartate aminotransferase, lactate dehydrogenase, creatine kinase 46
- 47. The current definition of FUO (Cont..) Antinuclear antibodies, and rheumatoid factor Urinalysis Culture: blood cultures (3 negative cultures) and urine culture 47
- 48. Etiology of FUO ▰ Infections (36%) - This accounts for majority of FUO cases. ▰ Neoplasms (19%) - lymphoma, leukemia, myeloma, renal, colon & liver Ca ▰ Non-infectious Inflammatory Diseases (19%) - connective tissue disorders like rheumatoid arthritis, SLE etc. ▰ Miscellaneous Causes (19%) – Granulomatous diseases, inherited & metabolic diseases etc. ▰ Undiagnosed cases (7%). 48
- 49. Infectious causes of fever of unknown origin 49 Bacterial causes Localized pyogenic infections Systemic bacterial infections Appendicitis Cholangitis Cholecystitis Localized abscess Mesenteric lymphadenitis Osteomyelitis Pelvic inflammatory disease Sinusitis Suppurative thrombophlebitis Intravascular infections Mycobacterial infections Typhoid fever Rickettsial infections Melioidosis Listeriosis Bartonellosis Actinomycosis and Nocardiosis Spirochete infections: Syphilis Lyme disease Relapsing fever Leptospirosis
- 50. Infectious causes of fever of unknown origin (Cont..) 50 Non-bacterial causes Viral infections Parasitic infections Fungal infections Cytomegalovirus and EBV infection Coxsackie virus group B infection Viral hepatitis HIV infection HSV infection Dengue West Nile virus infection Colorado tick fever Hantavirus infection Parvovirus infection Malaria Amoebiasis Leishmaniasis Chagas’ disease Toxoplasmosis Strongyloidiasis Echinococcosis Schistosomiasis Toxocariasis Aspergillosis Mucormycosis Blastomycosis Histoplasmosis Coccidioidomycosis Paracoccidioidomyc osis Candidiasis Cryptococcosis Pneumocystis infection Sporotrichosis
- 51. Laboratory Diagnosis- Specimen Collection ▰ Prior to specimen collection, a complete clinical history (including details of travel, immunization, exposure to any other patients) and physical examination should be carried out - may be helpful in choosing the appropriate specimen 51
- 52. Laboratory Diagnosis - Microscopy ▰ Blood microscopy ▰ Stool wet mount ▰ Gram stain of pus, sputum and other specimens ▰ Ziehl-Neelsen stain for M. tuberculosis. ▰ PAS or GMS stain 52
- 53. Laboratory Diagnosis - Culture ▰ Blood culture - typhoid fever, brucellosis ▰ Culture on Lowenstein Jensen medium - M. tuberculosis ▰ Culture of pus and exudate specimen from the abscesses ▰ Sabouraud dextrose agar (SDA) culture - fungal isolation ▰ Cell line culture 53
- 54. Laboratory Diagnosis - Serological Tests ▰ ELISA and rapid tests for viral diseases - hepatitis B and C, HIV, CMV, EBV infections, etc. ▰ Standard agglutination test: For brucellosis ▰ Microscopic agglutination test: For leptospirosis ▰ Cold agglutination test: For Mycoplasma ▰ Weil Felix test: For rickettsial diseases 54
- 55. Laboratory Diagnosis - Serological Tests (Cont..) ▰ Paul-Bunnell test: For infectious mononucleosis ▰ Widal test: For typhoid fever ▰ Microimmunofluorescence test for chlamydial infections ▰ Rheumatoid arthritis (RA) factor: For rheumatoid arthritis 55
- 56. Laboratory Diagnosis - Molecular Tests ▰ PCR can be carried out to amplify the specific genes 56
- 57. Laboratory Diagnosis - Other Tests ▰ Complete blood count: Increased neutrophil count indicates pyogenic infections ▰ Raised ESR (erythrocyte sedimentation rate) ▰ Histopathological examinations of the biopsies obtained from tumors may suggest the underlying etiology 57
- 58. Laboratory Diagnosis - Other Tests (Cont..) ▰ Imaging methods: Chest X-ray (for diagnosis of tuberculosis) and CT or MRI scan to identify the malignant tumors and their extension ▰ ECG and echocardiography: Rheumatic fever and IE 58
- 60. List of microorganisms causing anemia 60 Iron deficiency anemia It occurs due to blood loss, which occurs as a result of infection with various agents, leading to microcytic hypochromic anemia. Hookworm (Necator americanus and Ancylostoma duodenale) Trichuris trichiura Schistosoma species Hemolytic anemia It occurs due to destruction of RBCs. The various infectious agents include: Malaria (Plasmodium falciparum) Babesia microti Bartonella bacilliformis Clostridial sepsis (Clostridium perfringens) Infectious mononucleosis (Epstein-Barr virus) Hepatitis A virus
- 61. List of microorganisms causing anemia (Cont..) 61 Megaloblastic anemia It is caused by a parasite, Diphyllobothrium latum It causes dissociation of vitamin B12- intrinsic factor complex with in the gut lumen, which leads to decreased absorption of vitamin B12 in ileum. Aplastic anemia Aplastic anemia occurs as a result of bone marrow dysfunction (or failure) leading to a normocytic normochromic type of anemia. This can occur due to infection with various agents such as: M.tuberculosis , Rickettsial infections Leishmania donovani , Cytomegalovirus (CMV) Epstein-Barr virus , Varicella-zoster virus Parvovirus B19 (aplastic crisis in patients with chronic hemolytic anemia) Human immunodeficiency virus (HIV) , Human herpesvirus 6 (HHV-6) Hepatitis C virus
- 62. Questions: ▰ Q1. Examples of intermittent bacteremia: a. Brushing teeth b. Septic shock c. Endocarditis d. Undrained abscess 62
- 63. Questions: ▰ Q2. Which of the following is a component of qSOFA score: a. Altered mentation b. Respiratory system—PaO2/FiO2 c. Cardiovascular—Mean arterial pressure (MAP) d. Central nervous system—Glasgow coma scale score 63
- 64. Questions: ▰ Q3. Infections causing megaloblastic anemia: a. Babesia microti b. Diphyllobothrium latum c. Bartonella bacilliformis d. Leishmania donovani 64
- 65. THANK YOU