

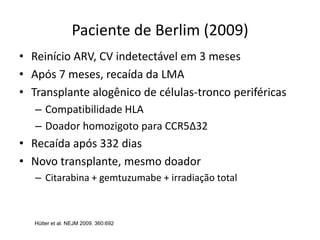
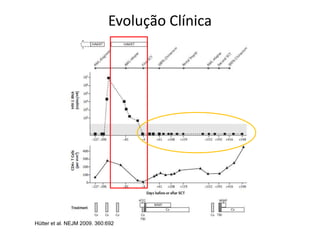
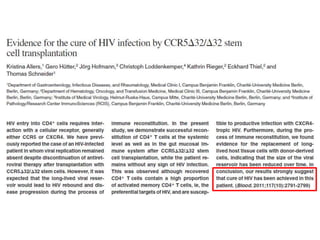
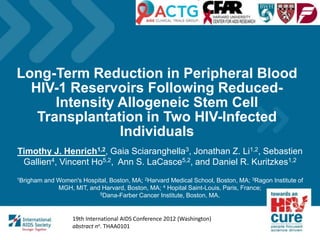
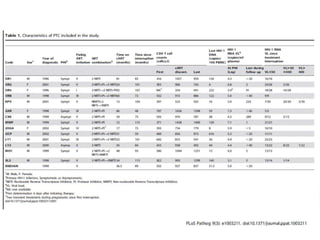
![Estimativas mundiais para crianças e adultos 2011
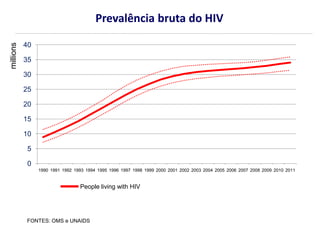
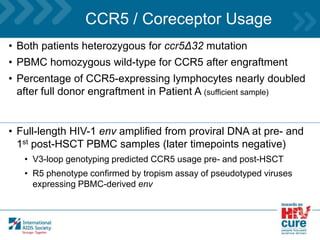
Pessoas com vivendo com HIV 34,0 milhões [31,4 –35.9]
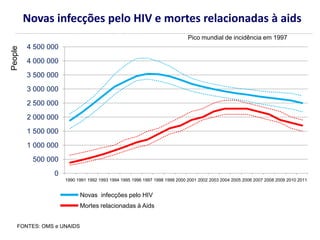
Novas infecções pelo HIV em 2011 2,5 milhões [2,2 –2,8 ]
Óbitos devidos ao HIV em 2011 1,7 milhões [1,5 million–1,9 ]
FONTES: OMS e UNAIDS](https://image.slidesharecdn.com/curafuncionaldohiv-130616162613-phpapp01/85/Dr-Celso-Ferreira-Ramos-Filho-Cura-funcional-do-HIV-4-320.jpg)
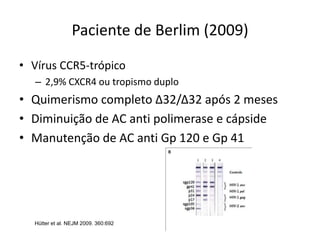
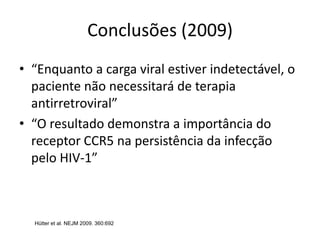
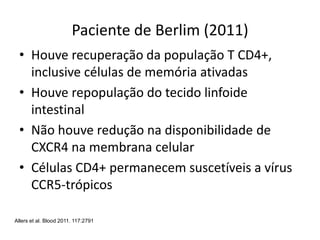
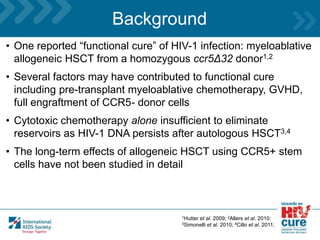
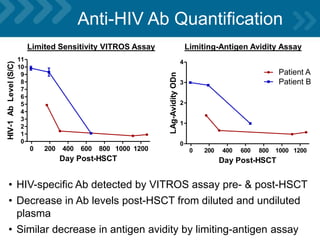
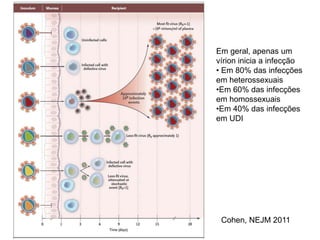
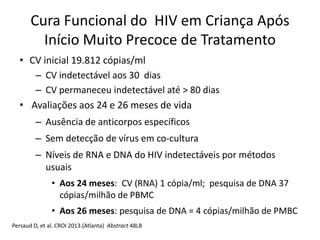
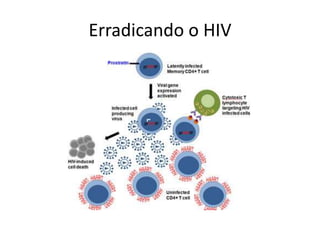
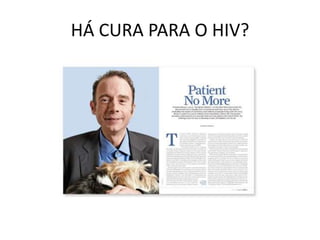
![Total: 34,0 milhões [31,4 milhões – 35,9 milhões]
Western &
Central Europe
900 000
[830 000 – 1.0 million]
Middle East & North Africa
300 000
[250 000 – 360 000]
Sub-Saharan Africa
23.5 million
[22.1 million – 24.8 million]
Eastern Europe
& Central Asia
1.4 million
[1.1 million – 1.8 million]
South & South-East Asia
4.0 million
[3.1 million – 5.2 million]
Oceania
53 000
[47 000 – 60 000]
North America
1.4 million
[1.1 million – 2.0 million]
Latin America
1.4 million
[1.1 million – 1.7 million]
East Asia
830 000
[590 000 – 1.2 million]
Caribbean
230 000
[200 000 – 250 000]
Prevalência bruta estimada do HIV (adultos e crianças) 2011
FONTE: OMS e UNAIDS](https://image.slidesharecdn.com/curafuncionaldohiv-130616162613-phpapp01/85/Dr-Celso-Ferreira-Ramos-Filho-Cura-funcional-do-HIV-5-320.jpg)
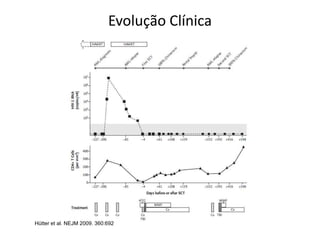
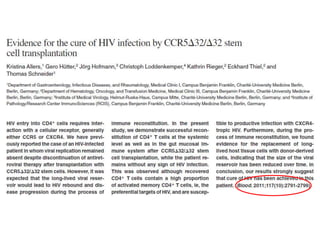
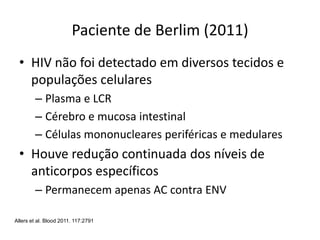
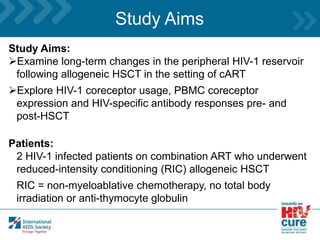
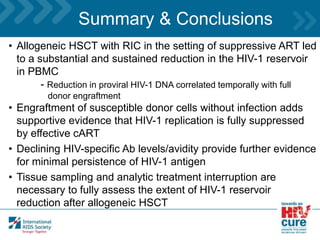
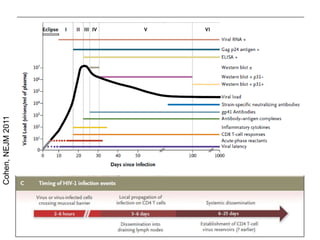
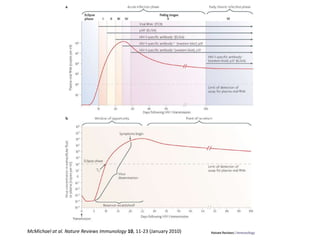
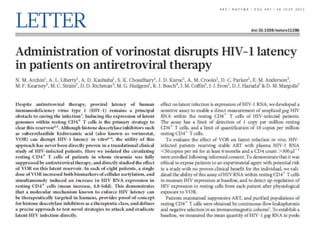
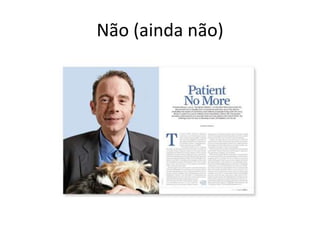
![Incidência bruta estimada do HIV (adultos e crianças) 2011
Western &
Central Europe
30 000
[21 000 – 40 000]
Middle East & North Africa
37 000
[29 000 – 46 000]
Sub-Saharan Africa
1.8 million
[1.6 million – 2.0 million]
Eastern Europe
& Central Asia
140 000
[91 000 – 210 000]
South & South-East Asia
280 000
[170 000 – 460 000]
Oceania
2900
[2200 – 3800]
North America
51 000
[19 000 – 120 000]
Latin America
83 000
[51 000 – 140 000]
East Asia
89 000
[44 000 – 170 000]
Caribbean
13 000
[9600 – 16 000]
Total: 2.5 million [2.2 million – 2.8 million]
FONTE: OMS e UNAIDS](https://image.slidesharecdn.com/curafuncionaldohiv-130616162613-phpapp01/85/Dr-Celso-Ferreira-Ramos-Filho-Cura-funcional-do-HIV-6-320.jpg)

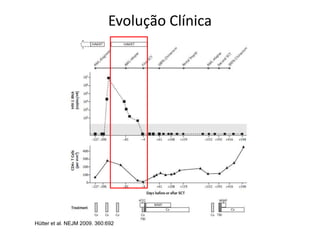
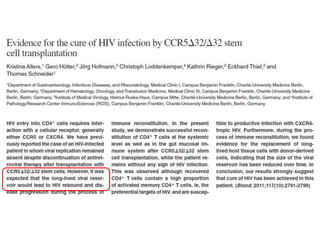
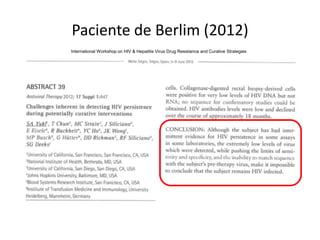
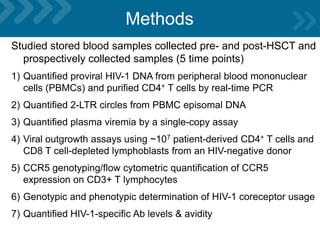
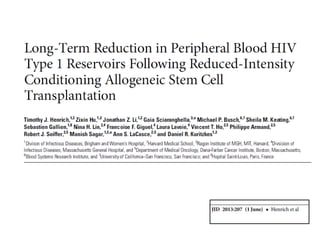
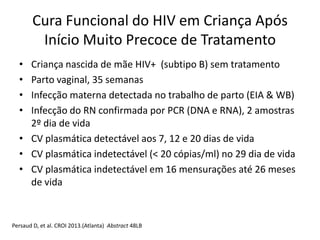
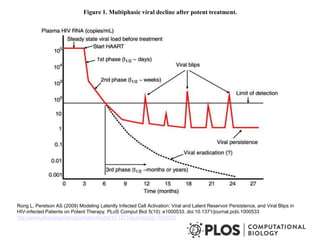
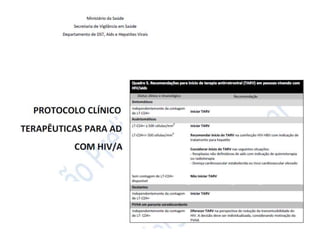
![clinicaloptions.com/hiv
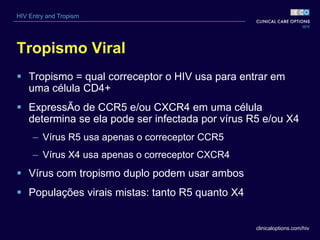
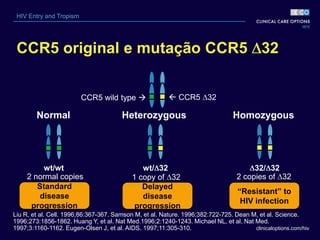
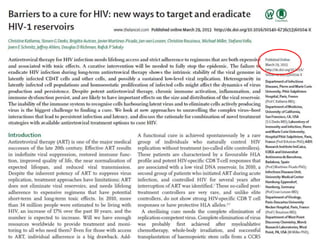
HIV Entry and Tropism
Pacientes homozigotos ou
heterozigotos para CCR5 32
Homozigotos
– ~ 1% da etnia branca[1]
– Sem moléculas CCR5 na superfície de células CD4+ [2,3]
– Resistentes a vírus R5
– Suscetíveis aos vírus X4
– Função imune relativamente normal
Heterozigotos
– 10% a 15% da etnia branca [1]
– Menos moléculas CCR5 na superfície celular[4]
– Função imune normal[2]
1. McNicholl JM, et al. Emerg Infect Dis. 1997;3:261-271. 2. Liu R, et al. Cell. 1996;86:367-367. 3. Samson
M, et al. Nature. 1996;382:722-725. 4. Wu L, et al. J Exp Med. 1997;185:1681-1691.](https://image.slidesharecdn.com/curafuncionaldohiv-130616162613-phpapp01/85/Dr-Celso-Ferreira-Ramos-Filho-Cura-funcional-do-HIV-15-320.jpg)
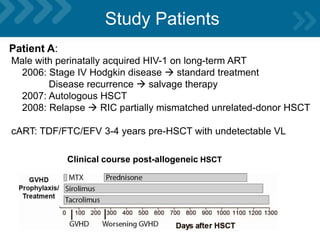
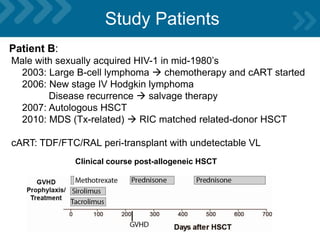
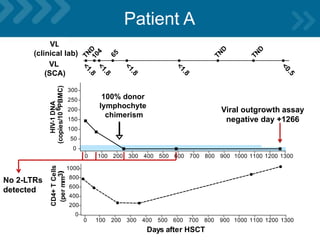
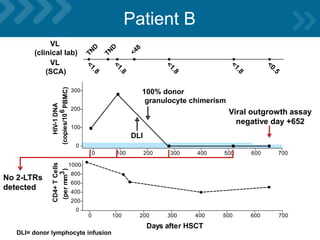
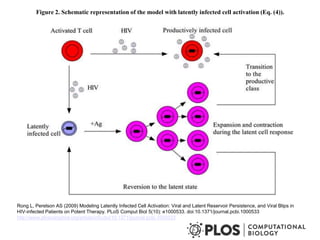
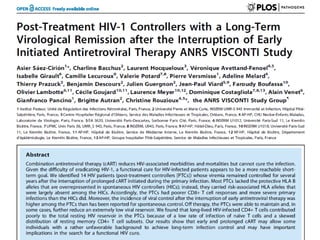
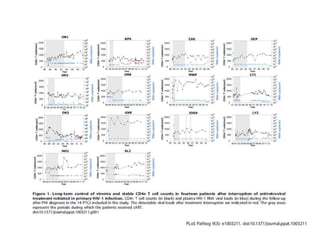



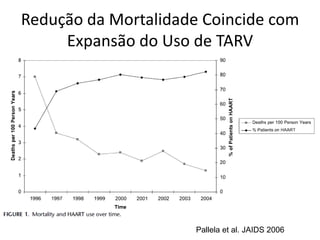
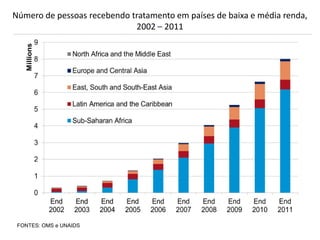
The document discusses the functional cure for HIV, highlighting the significant reduction in mortality due to the increased use of antiretroviral therapy (ART) and presenting global statistics on HIV prevalence and incidence for the year 2011. It details the role of the CCR5 gene mutation in HIV infection susceptibility and explores case studies, particularly focusing on the Berlin Patient, who underwent stem cell transplantation from a CCR5-delta32 homozygous donor, suggesting a potential path toward a functional cure for HIV. Additionally, the study outlines the results of ongoing research into HIV reservoirs and their implications for treatment outcomes.



























































































