#4 In summary all RRT can be classified as intermittent or continuous. Availability of techniques and expertise among the staff are important considerations in the choice of renal replacement modality in the ICU. The application of IHD needs the nursing and technical expertise of a dialysis team, whereas CRRT is technically less demanding and can be performed by trained ICU staff.
The basic principle for all treatment modalities except PD, is the same,they are all extra-corporeal blood purification. Blood is removed from the patient, pumped through a dialysis or hemo-filter and returned to the patient following removal of excess water and metabolic waste. The filter performs many of the functions of the kidney's nephron unit, hence, it is referred to as an "artificial kidney".
PD is an intra-corporeal blood purification, meaning that contrary to IHD and CRRT, no blood ever leaves the body of the patient.A thin membrane, the peritoneum, lines the abdominal cavity, and all the organs contained in it, in peritoneal dialysis the peritoneum serves as the dialysis membrane.
#5 Drs. Bellomo, Ronco and Mehta defined Continuous renal replacement therapy (CRRT) as any extracorporeal blood purification therapy intended to substitute for impaired renal function over an extended period of time and applied for or aimed at being applied for 24 hours/day.
It is also referred to as slow continuous renal replacement therapy. Treatments are usually performed by a critical care nurse over a 24-hour period, the duration of therapy varying from days to weeks depending on individual patient requirements.
#10 ADQI (Acute Dialysis Quality Initiative) is a process initiated by a group of physicians from different part of the world, with the objective to seek consensus and evidence and establish guidelines in the field of acute renal failure.
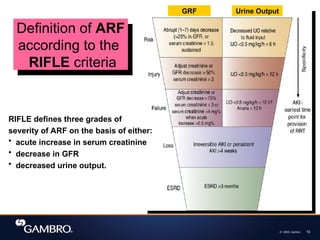
They have proposed the RIFLE classification as a definition of ARF (acute renal failure). RIFLE defines three grades of severity of ARF on the basis of either an acute increase in serum creatinine, decrease in GFR or decreased urine output.
#12
AZOTEMIA
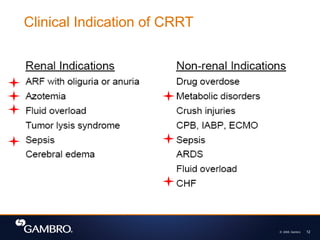
Azotemia is a condition where the patient's blood contains uncommon levels of urea, creatinine, and other compounds rich in nitrogen. Azotemia is also one clinical characteristic of a wider condition known as uremia, which includes other conditions such as acidosis, anemia, hyperkalemia, hypertension, hypocalcemia, etc.
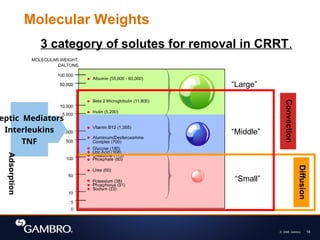
#18 The solutes, or molecules, that clinicians target for removal and maintenance during therapy come in different sizes, the weights of which are expressed in daltons. These solutes are classified into small, medium, or large depending on their molecular weight. For example, urea and creatinine, which are molecules usually used as markers for efficiency of dialysis treatment, are considered small.
Vit. B12, which is not a molecule targetted for removal but is usually used as a marker for middle molecules, are considered a middle molecule. Septic mediators, interleukins and TNF, fall in this category.
Beta-2 microglobulins, a large molecule, has been described as the cause for microinflammatory diseases for chronic dialysis patients, and is usually used to describe the efficiency of a hemofilter membrane. Whereas albumin is a molecule too large to pass through the pores of a hemofilter membrane.
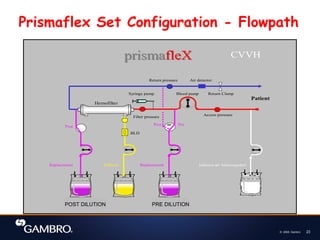
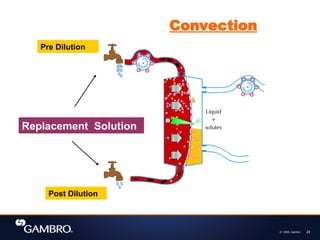
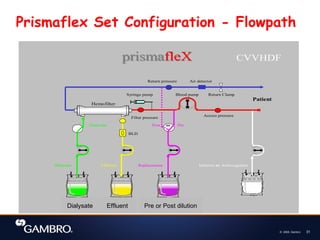
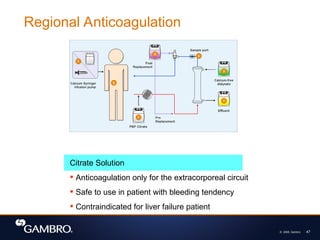
#24 From the animation, you see also that replacement fluid can be added at 2 points:
1st is when replacement fluid is added to the blood before it enters the haemofilter. This is known as pre dilution.
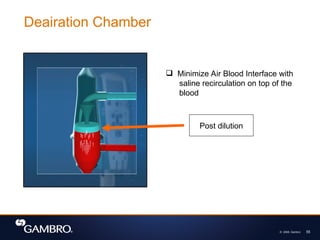
2nd is when replacement fluid is added into blood after it leaves the heamofilter. This is known as post dilution.
( Please do refer to the diagram at the same time you explain)
Ask: Why is there a need for Pre and Post Dilution?
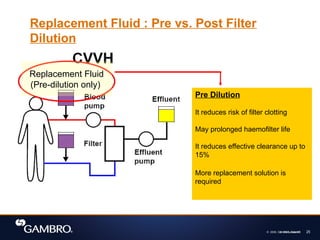
#25 In pre dilution, blood is diluted before it enters the haemodfilter. ( please refer to the pink colour box when reading.)
Ask: What are the advantages of pre dilution?
1st - It reduces risk of filter clotting
2nd - May prolonged haemofilter life
However, the disadvantages are:
It reduces effective clearance up to 15%, and hence more replacement solution required to improve clearance
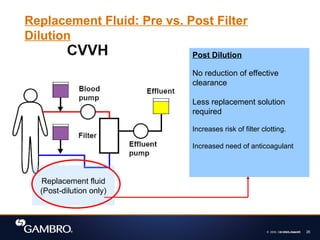
#26 In post dilution, replacement fluid is added to patient’s blood after it leave the heamofilter. ( please refer to the pink colour box when reading.)
Ask: What are the advantages of post dilution?
There is no reduction of effective clearance and hence less replacement solution is required to get the same amount of clearance.
However, the disadvantages are:
It increases the risk of filter clotting and hence increases need of anticoagulant
#29 Read from the yellow box
Picture
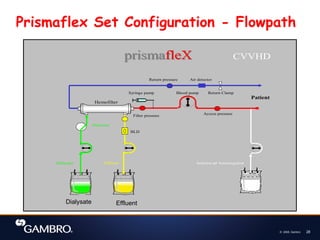
In this haemofilter animation, you can see that Dialysate solution is exposed to the blood across the semi permeable membrane.
Important! Dialysate solution is not added to the blood. It is separate from the blood by the semi permeable membrane.
The dialysate solution flows in a counter current direction to the blood. This is to maximize the diffusion capability.
Go to next slide
#32 From the animation, we see that in CVVHDF; both convection and diffusion are used to remove waste.
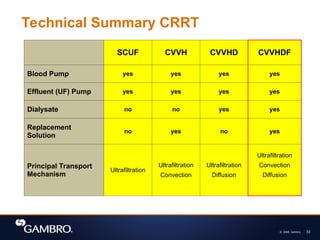
#33 This slide summarises the different technique used in CRRT:
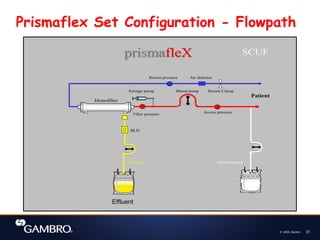
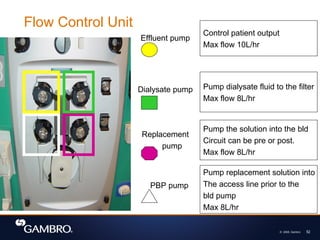
SCUF Slow continuous ultrafiltration. Requires blood and effluent pumps. Pumps used to generate hydrostatic pressure. No dialysate or replacement solutions are required. In this mode, CRRT fluid removal rates up to 2 litres/hr can be achieved.
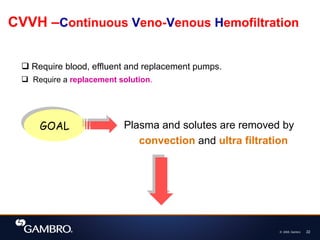
CVVH Continuous veno-venous hemofiltration. Requires use of blood, effluent and replacement pumps. Dialysate solution is not required. Plasma water and solutes are removed by ultrafiltration and convection .
CVVHD Continuous veno-venous hemodialysis. Requires the use of blood, effluent and dialysis pumps. Replacement solution is not required. Plasma water and solutes are removed by ultrafiltration and diffusion .
CVVHDF Continuous veno-venous hemodiafiltration. Requires the use of blood, effluent, dialysate and replacement pumps. Both dialysate solution and replacement solution are used. Plasma water and solutes are removed by ultrafiltration convection and diffusion.
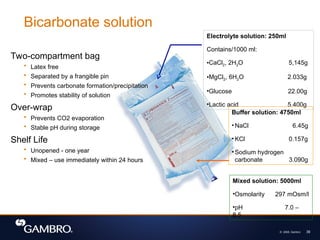
#39 As you know, bicarbonate is the most physiologically compatible and therefore is the preferred solution for patients. It comes in a two-compartment plastic bag, which is latex free. The contents of each compartment is separated by a red colored frangible pin.
The large compartment contains 4750ml of solution composed of sodium hydrogen carbonate and water. This solution has a pH of 8.3.
The small compartment has 250ml of solution which contains electrolytes such as NaCl, variable K+ and Ca+, MgCl, Lactic Acid and water. Separating the carbonate from Ca and Mg prevents carbonate formation and precipitation. In addition, the over-wrap prevents carbonate evaporation and therefore promotes the stability of the solution during storage.
Unmixed, the solution has a shelf life of one year. Gambro recommends that the solution is used immediately after mixing the contents of the two compartments, up to 24hours after removing the overwrap. No stability test has been done for other additives to the solutions.
#45 The role of anticoagulation during CRRT is to minimize the effects of membrane exposure to blood and maintain the functional integrity of the filter and the patency of the circuit. The ultimate goal is to minimize clotting of the extracorporeal circuit without systemically anticoagulating the patient while minimizing the systemic side effects of anticoagulation. There are two types of anticoagulation strategies often used to obtain this goals, either by systemic or regional anticoagulation. Systemic anticoagulation involves anticoagulating both the extracorporeal circuit and the patient. Regional anticoagulation refers to anticoagulation restricted to the extracorporeal circuit.
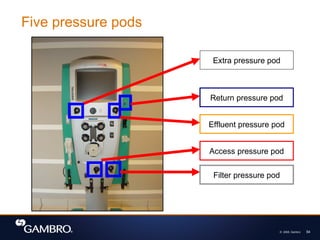
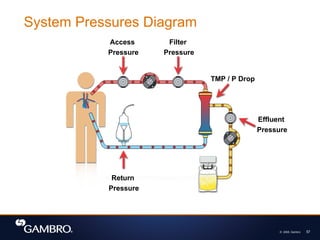
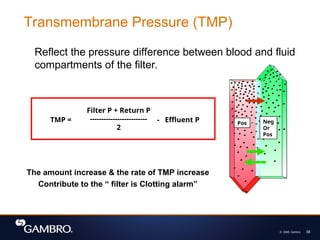
#58 TMP or Trans Membrane Pressure is the pressure exerted on the filter membrane, it reflects the pressure difference between the fluid and blood compartment of the filter.
Most CRRT Systems automatically calculates the TMP of the membrane with this formula, taking into account the filter pressure (pressure at the blood inlet of the filter), the return pressure and the effluent pressure (pressure at the fluid outlet). An increase in the TMP may signify protein coating on the blood side of the membrane, or clotting of the fibers.
The TMP in the filter data is described in mmHg/kPa. A Pascal is a unit of pressure equal to one Newton per square meter. A Newton is the international standard unit of force. A maximum TMP is specified for each hemofilter. The bigger the surface area of the filter, the more room to increase the blood flow before reaching the maximum TMP.
If all the alarm systems in a machine fails, and the TMP was allowed to go beyond the maximum limit, what do you think would happen to the membrane?
What does a negative TMP mean? (backfiltration, or the filter is much bigger than the programmed fluid removal)
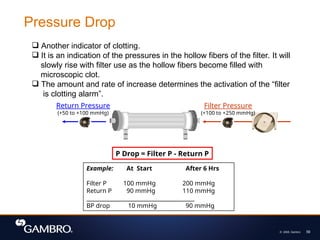
#59 Blood pressure drop of a hemofilter is usually indicated in the filter data for CRRT. It is a calculated value using the measured pressure as the blood is entering and leaving the filter, at a certain blood flow rate with the specified UFR in post-dilution mode. The bigger the BP drop, the more susceptible the hemofilter is to clotting with higher UFR. The bigger the surface area of the hemofilter, the lower the BP drop would be, therefore, a bigger filter would allow higher UFR with lower risk of clotting.