The document discusses coronary artery disease and myocardial infarction. It provides details on the topics including:
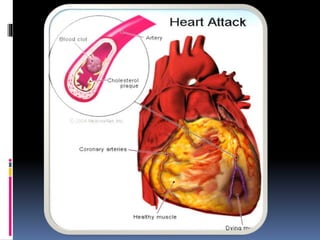
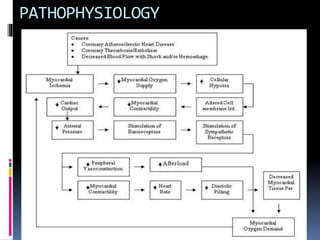
- Coronary artery disease is caused by a narrowing of the arteries that limits blood supply to the heart, often due to atherosclerosis. This can damage the heart muscle over time.
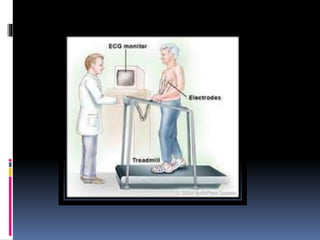
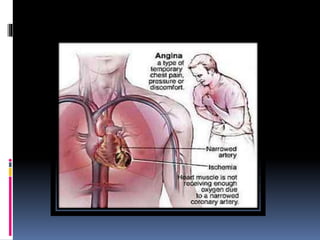
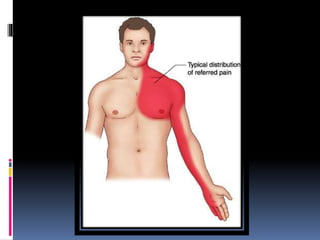
- Risk factors include conditions like high cholesterol, smoking, diabetes and high blood pressure. Symptoms include chest pain and discomfort. Diagnosis involves tests like ECGs, stress tests and angiography.
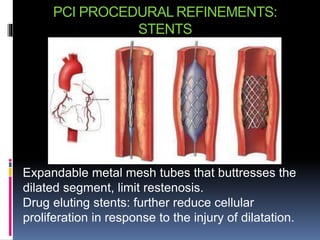
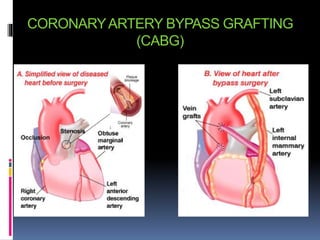
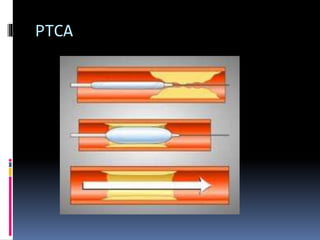
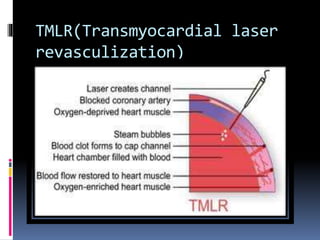
- Treatment involves medications to reduce symptoms, risk factors and complications as well as procedures like angioplasty and bypass surgery to reopen blocked arteries. Myocardial infarction is heart muscle damage from reduced blood flow and can be a