The document discusses a study aimed at predicting heart disease by integrating mental health indicators with traditional cardiovascular risk factors using machine learning models, particularly focusing on age and gender distinctions. It highlights the challenges faced by low and middle-income countries in accessing advanced diagnostic tools and emphasizes the importance of considering psychological factors in predictive models. The study employs various machine learning classifiers, aiming to enhance predictive accuracy and improve healthcare access through future developments such as wearable device integration.

![INTRODUCTION
Cardiovascular diseases (CVDs) are the leading global cause of death,
responsible for 17.9 million deaths annually [1].
Low and middle-income countries face critical challenges due to limited
healthcare resources.
Advanced diagnostic tools (e.g., angiography, ECG) are often inaccessible due to
high costs and need for specialized professionals [2].
Traditional prediction models focus only on physical factors (e.g., cholesterol,
blood pressure, age) [3].
Mental health factors like stress, sleep duration, and working hours, which impact
cardiovascular health, are often overlooked [2].](https://image.slidesharecdn.com/confrenceppt1-250119172901-c30d5f34/85/confrence_ppt-1-confrence_ppt-1confrence_ppt-1-pptx-2-320.jpg)
![INTRODUCTION
Machine learning provides a cost-effective approach to predicting heart disease
risks [4].
Study integrates psychological factors like stress, work hours, and sleep into
predictive models.
Cleveland Heart Disease dataset enriched with synthetic mental health features for
analysis.
Personalized models based on age (<40 vs. ≥40) and gender were explored.](https://image.slidesharecdn.com/confrenceppt1-250119172901-c30d5f34/85/confrence_ppt-1-confrence_ppt-1confrence_ppt-1-pptx-3-320.jpg)
![LITERATURE REVIEW
• Mohan et al. [1], Highlighted the potential of hybrid machine learning models,
combining physical and psychological parameters, to improve predictive accuracy in
heart disease.
• Subahi et al. [5] Proposed the integration of stress levels, sleep patterns, and lifestyle
factors into datasets to enhance the prediction of heart disease.
• Yaqoob et al. [6], Identified fasting blood sugar as a critical predictor of heart disease,
but pointed out the limitations of models that exclude multi-dimensional health
factors, particularly psychological ones.
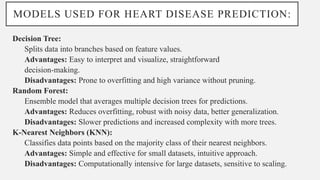
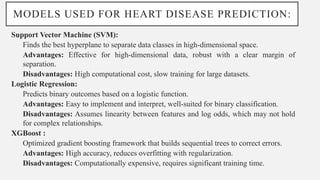
• Soni et al. [7] Demonstrated that advanced ML algorithms like Random Forest and
XGBoost outperform traditional models in predictive accuracy, effectively capturing
non-linear relationships between variables, but face challenges in model
explainability for clinical acceptance.](https://image.slidesharecdn.com/confrenceppt1-250119172901-c30d5f34/85/confrence_ppt-1-confrence_ppt-1confrence_ppt-1-pptx-4-320.jpg)
![PROPOSED METHODOLOGY
• Dataset Details: Cleveland Heart Disease Dataset (303 records, UC Irvine ML
Repository) [8].
• Attributes: Age, Sex, Cholesterol, Blood Pressure, Exercise-Induced Angina, etc.
• Synthetic Features Added: Stress Level (1–10), Sleep Duration (4–9 hours/day),
Work Hours (20–70 hours/week).
• Age Group: Young (<40 years) and Old (≥40 years)
• Data Pre-processing: Converted categorical variables (e.g., Sex, Chest Pain Type)
into numeric.
• Handled missing values via imputation or exclusion.
• Normalized data for scale-sensitive models (e.g., XGBoost, KNN).
• Feature Engineering: Key features identified using Random Forest importance.
• Experimented with top 2 and top 4 features for better performance.](https://image.slidesharecdn.com/confrenceppt1-250119172901-c30d5f34/85/confrence_ppt-1-confrence_ppt-1confrence_ppt-1-pptx-6-320.jpg)
![REFERENCES
[1 [7] P. Soni and R. Sharma, "Deep Learning Models for Heart Disease
Prediction: A Review," Computers in Biology and Medicine, vol. 147, p.
105436, 2022.
[8] Psychogyios, K., Ilias, L., Askounis, D.: Comparison of missing data
imputation methods using the Framingham heart study dataset. In: 2022
IEEE-EMBS International Conference on Biomedical and Health
Informatics (BHI), pp. 1–5 (2022)](https://image.slidesharecdn.com/confrenceppt1-250119172901-c30d5f34/85/confrence_ppt-1-confrence_ppt-1confrence_ppt-1-pptx-12-320.jpg)