This document summarizes Dr. Laurie Powell's presentation about problem solving interventions following brain injury. Some key points:
1. Dr. Powell directs the Center on Brain Injury Research and Training (CBIRT) at the University of Oregon, which conducts research and training to help those with traumatic brain injury (TBI).
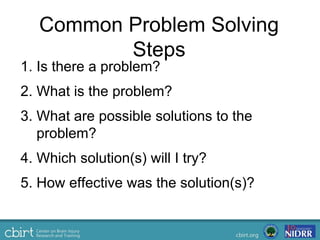
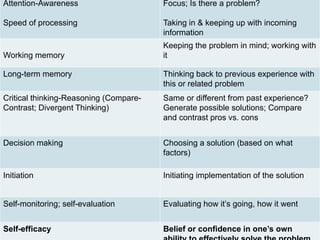
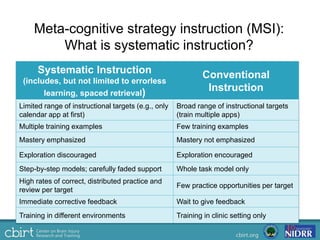
2. CBIRT's research focuses on systematic instruction techniques and meta-cognitive strategy instruction to support improved problem solving following TBI.
3. Their current project involves developing an integrated web-based and mobile app intervention called "ProSolv" to help individuals with TBI generalize problem solving strategies to everyday life.