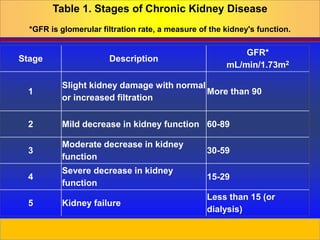
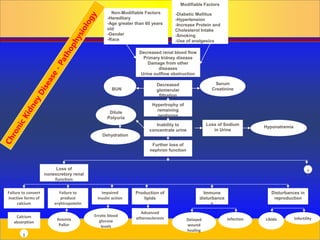
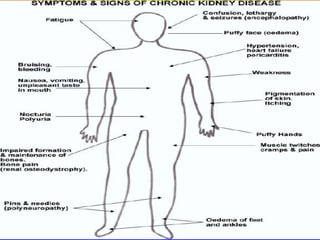
Chronic kidney disease is progressive and irreversible damage to the nephrons and glomeruli of the kidneys. Major causes include diabetes, high blood pressure, glomerulonephritis, and polycystic kidney disease. As kidney function declines, waste products accumulate in the blood and patients experience symptoms like fatigue, itchy skin, and fluid retention. Kidney function is staged based on glomerular filtration rate, and end-stage renal disease occurs when kidney function is less than 15%. Treatment options include modifying risk factors, dietary restrictions, dialysis, and kidney transplantation.

![Prepared by D. Chaplin
Diffusion - movement of solutes (particles) from an
area of > concentration to area of < concentration
[Remove urea, creatinine, uric acid and electrolytes,
from the blood to the dialystate bath] RBC, WBC,
Large plasma proteins do not go through
Ultrafiltration – Water and fluid removed when the
pressure gradient across the membrane is created,
by increase pressure in the blood compartment &
decrease pressure in the dialysate compartment
Osmosis - movement fluid from an area of < to >
concentration of solutes (particles)
Osmosis-Diffusion-Ultrafiltration](https://image.slidesharecdn.com/chronic20kidney20diseass-240210183754-bfc79638/85/chronic-20kidney-20diseass-ppt-BY-NATUNGA-RONALDx-20-320.jpg)




















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














