Download to read offline







































![Some dehydration
Administer ORS solution according to the amount recommended in Table 3.
Table 3. Approximate Amount of ORS Solution to Administer in the First 4 Hours
]
Age* <4
mo
4-11
mo
12-
23
mo
2-4 y 5-14
y
³ 15 y
Weight <5
kg
5-
7.9
kg
8-
10.9
kg
11-
15.9
kg
16-
29.9
kg
³ 30
kg
ORS
solution in
mL
200-
400
400-
600
600-
800
800-
1200
1200-
2200
2200-
4000
•Use the patient's age only when weight is unknown.](https://image.slidesharecdn.com/cholera-230628181639-b8207ccc/85/Cholera-ppt-50-320.jpg)












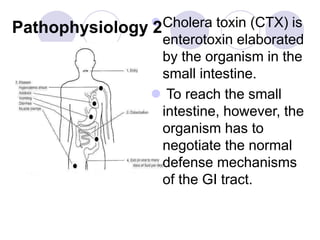
Cholera is a bacterial disease caused by Vibrio cholerae that causes severe watery diarrhea and dehydration. It occurs in outbreaks related to contaminated water supplies in areas with poor sanitation. Clinical presentation includes sudden onset of painless, copious watery diarrhea and vomiting leading to severe dehydration and death if untreated. Diagnosis is confirmed by identifying the bacteria in a stool sample. Treatment focuses on oral rehydration and intravenous fluids to replace fluid and electrolyte losses. Antibiotics are given to shorten the duration of illness and reduce spread.



































































