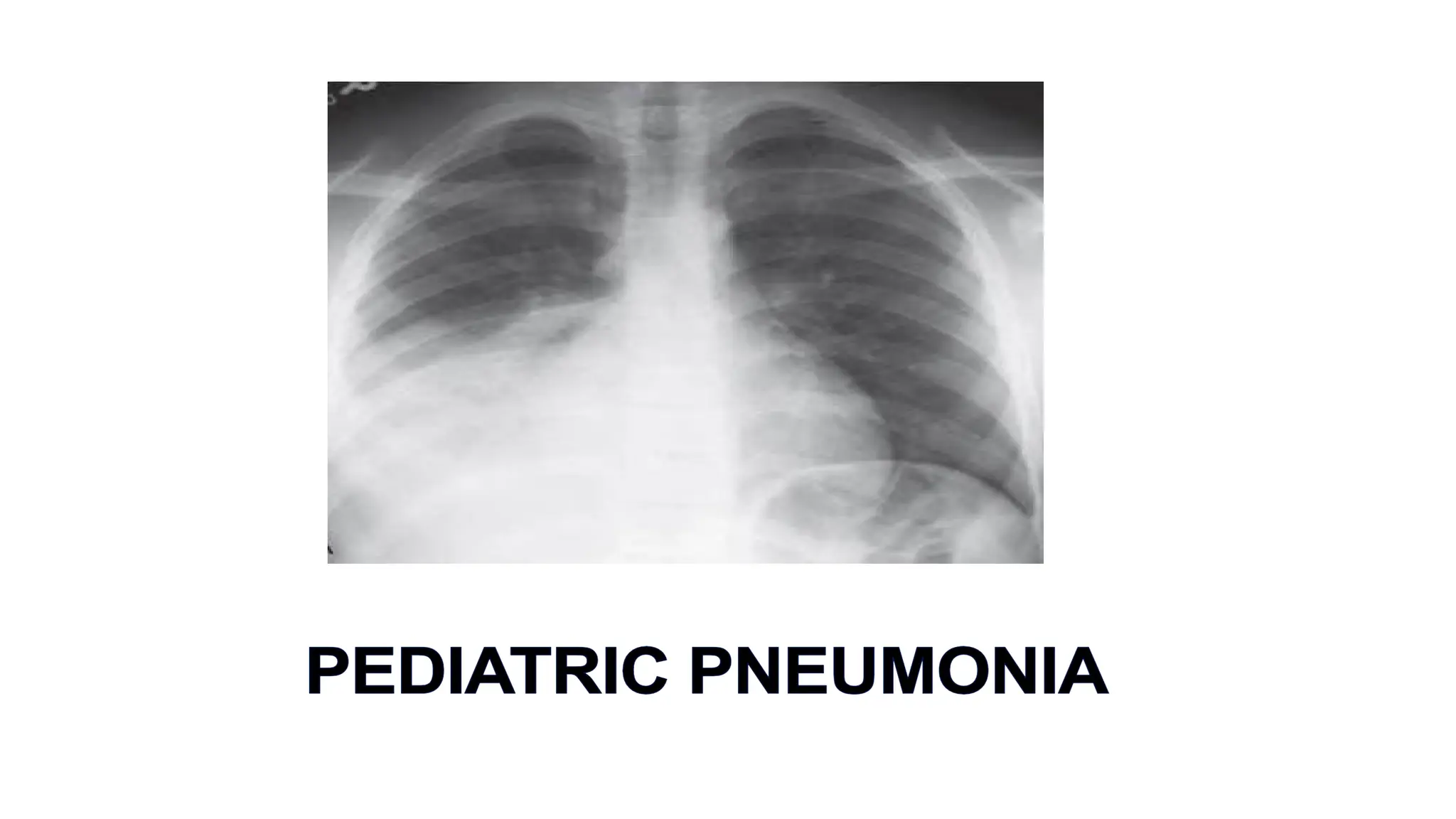
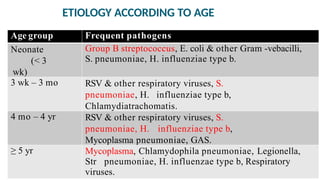
Pneumonia is a significant cause of under-five mortality, particularly in developing countries, with various risk factors including malnutrition and lack of immunization. The document outlines the clinical classification, etiology based on age, mode of transmission, clinical manifestations, and treatment approaches for pneumonia, along with necessary investigations and preventative measures. Complications and prognosis are discussed, emphasizing the importance of proper management and early intervention.