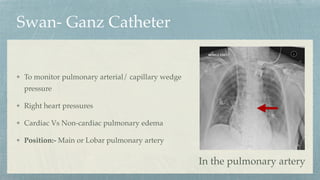
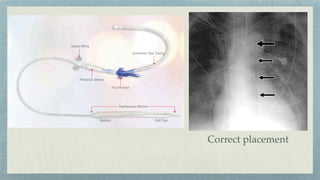
Swan- Ganz Catheter
Tomonitor pulmonary arterial/ capillary wedge
pressure
Right heart pressures
Cardiac Vs Non-cardiac pulmonary edema
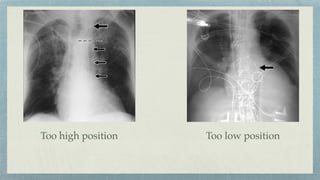
Position:- Main or Lobar pulmonary artery
In the pulmonary artery
11.
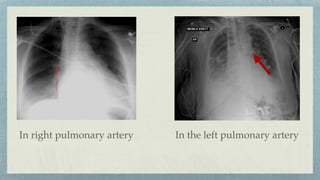
In the leftpulmonary artery
In right pulmonary artery
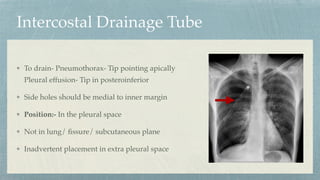
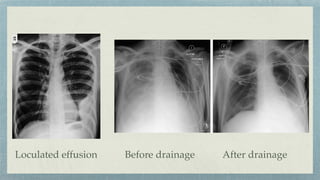
Intercostal Drainage Tube
Todrain- Pneumothorax- Tip pointing apically
Pleural effusion- Tip in posteroinferior
Side holes should be medial to inner margin
Position:- In the pleural space
Not in lung/
fi
ssure/ subcutaneous plane
Inadvertent placement in extra pleural space
18.
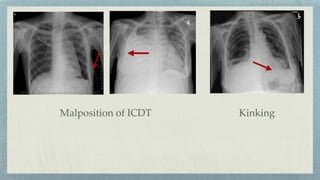
Complications:- Intra parenchymalpositioning
Pulmonary lacerations, hematoma, infarction, bronchopleural
fi
stula
Ineffective drainage: tube kinking, blood clot, pus, debris
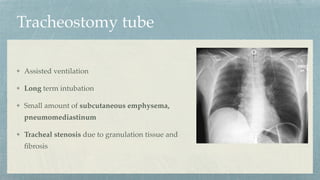
Tracheostomy tube
Assisted ventilation
Longterm intubation
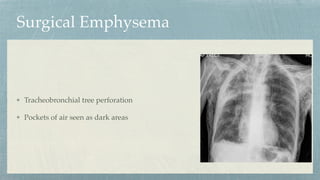
Small amount of subcutaneous emphysema,
pneumomediastinum
Tracheal stenosis due to granulation tissue and
fi
brosis
Intra Aortic BalloonPump
Patients with cariogenic shock
Ejection fraction <20%
Position- metallic tip in AP window
Distal to left subclavian artery
In
fl
ate- diastole
De
fl
ate- systole
Increases coronary
fl
ow
Decreases after load
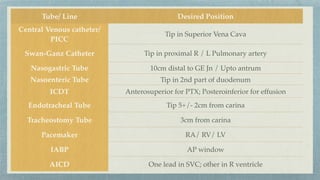
Tube/ Line DesiredPosition
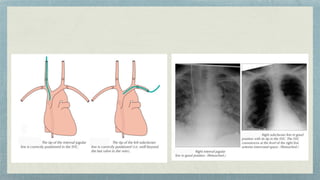
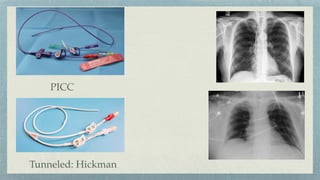
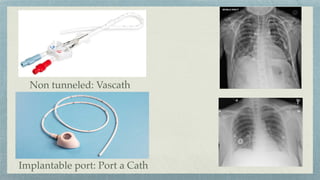
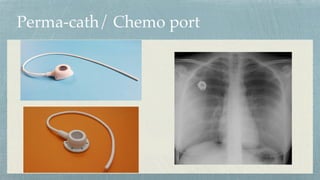
Central Venous catheter/
PICC
Tip in Superior Vena Cava
Swan-Ganz Catheter Tip in proximal R / L Pulmonary artery
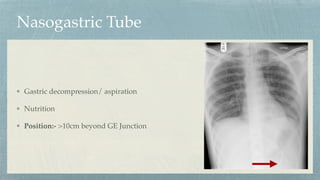
Nasogastric Tube 10cm distal to GE Jn / Upto antrum
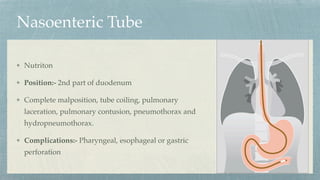
Nasoenteric Tube Tip in 2nd part of duodenum
ICDT Anterosuperior for PTX; Posteroinferior for effusion
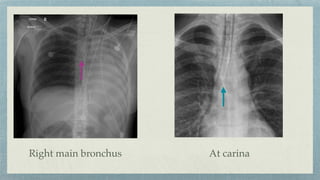
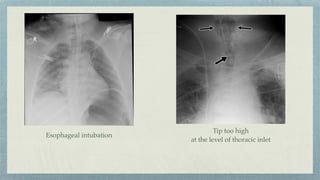
Endotracheal Tube Tip 5+/- 2cm from carina
Tracheostomy Tube 3cm from carina
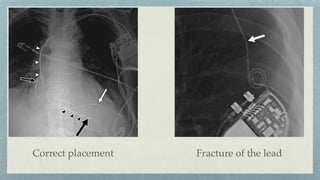
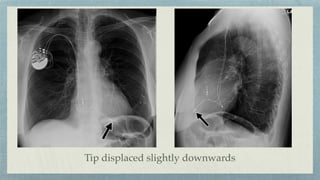
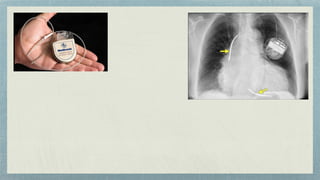
Pacemaker RA/ RV/ LV
IABP AP window
AICD One lead in SVC; other in R ventricle
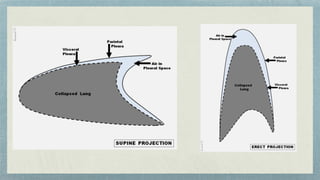
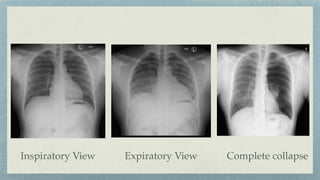
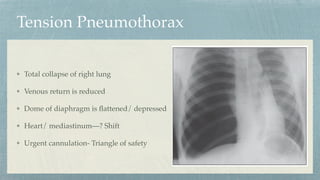
Tension Pneumothorax
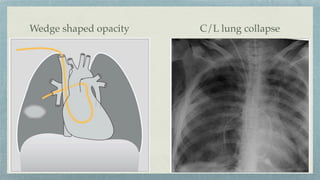
Total collapseof right lung
Venous return is reduced
Dome of diaphragm is
fl
attened/ depressed
Heart/ mediastinum—? Shift
Urgent cannulation- Triangle of safety
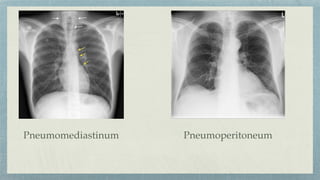
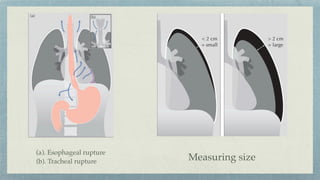
Pneumomediastinum
Causes- Alveolar rupturedue to mechanical
ventilation
Thoracic trauma
Tracheal/ Bronchial rupture
Extra thoracic sites:-
Vascular sheath in the neck
Retropharyngeal space
Submandibular space
Retropharyngeal space
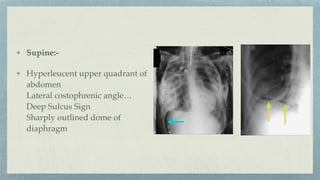
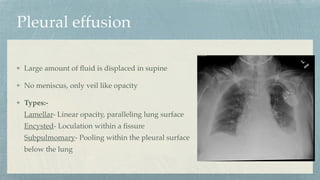
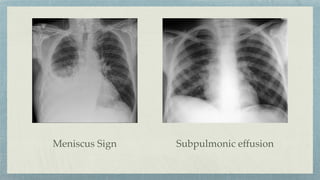
Pleural effusion
Large amountof
fl
uid is displaced in supine
No meniscus, only veil like opacity
Types:-
Lamellar- Linear opacity, paralleling lung surface
Encysted- Loculation within a
fi
ssure
Subpulmomary- Pooling within the pleural surface
below the lung
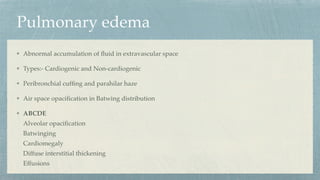
Pulmonary edema
Abnormal accumulationof
fl
uid in extravascular space
Types:- Cardiogenic and Non-cardiogenic
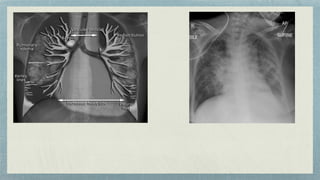
Peribronchial cuf
fi
ng and parahilar haze
Air space opaci
fi
cation in Batwing distribution
ABCDE
Alveolar opaci
fi
cation
Batwinging
Cardiomegaly
Diffuse interstitial thickening
Effusions






























![Chest_trauma types and management[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/malamulochesttrauma1-241126062258-4b388e87-thumbnail.jpg?width=640&height=640&fit=bounds)
![management of Chest_trauma for nursing [1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/malamulochesttrauma1-241127110255-71befbaa-thumbnail.jpg?width=640&height=640&fit=bounds)



















