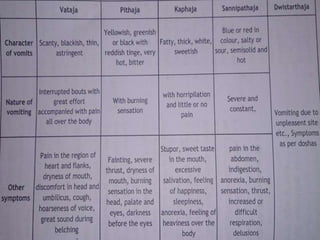
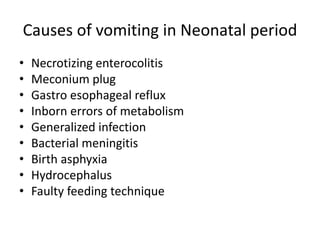
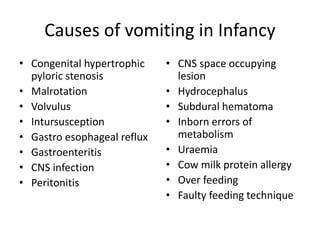
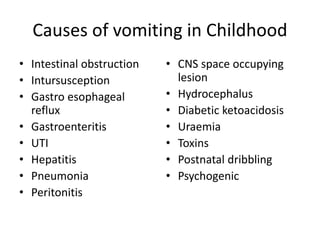
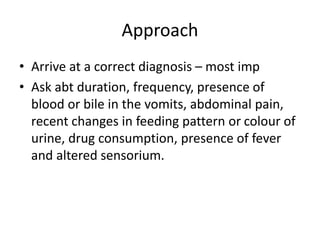
Chardi is defined as vomiting that covers the mouth in bouts and causes discomfort from body bending as doshas are expelled. It is caused by abnormal udana vayu moving doshas upwards. Treatment depends on the type but may include induced vomiting, herbal remedies, or fasting initially except in vata conditions. Approaching vomiting requires determining the cause through duration, presence of blood/bile, pain, recent changes, and symptoms to identify organic causes and site of lesion. Management treats the underlying cause and provides symptomatic relief and rehydration.