1. Cesarean section, also known as C-section, is the delivery of a baby through surgical incisions in the mother's abdomen and uterus after at least 28 weeks of gestation.
2. The rate of C-sections has been rising worldwide with over 30% of deliveries in the US being C-sections. The optimal C-section rate is considered to be between 5-15% as this provides the best maternal outcomes.
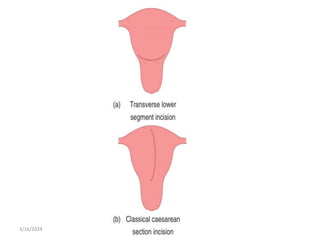
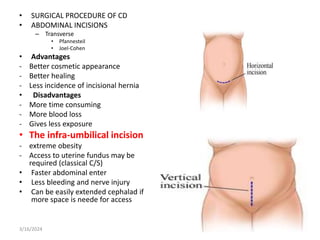
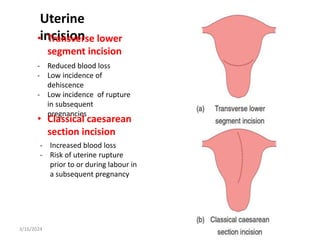
3. Common indications for C-section include previous C-section, breech or other malpresentation, failure to progress in labor, and suspected fetal compromise. Vertical incisions over the lower uterine segment carry more risks than transverse incisions.