This document discusses the importance of considering facial aesthetics in orthodontic treatment planning. It makes three key points:
1) Attaining and preserving optimal facial attractiveness is a primary goal of orthodontic treatment. However, correcting the bite does not always lead to improved facial traits and can sometimes decrease facial attractiveness if soft tissue outcomes are not considered.
2) Relying solely on cephalometric analysis of hard tissue structures to plan treatment can lead to esthetic problems, as soft tissue profiles vary greatly and are only partially dependent on underlying skeletal structures.
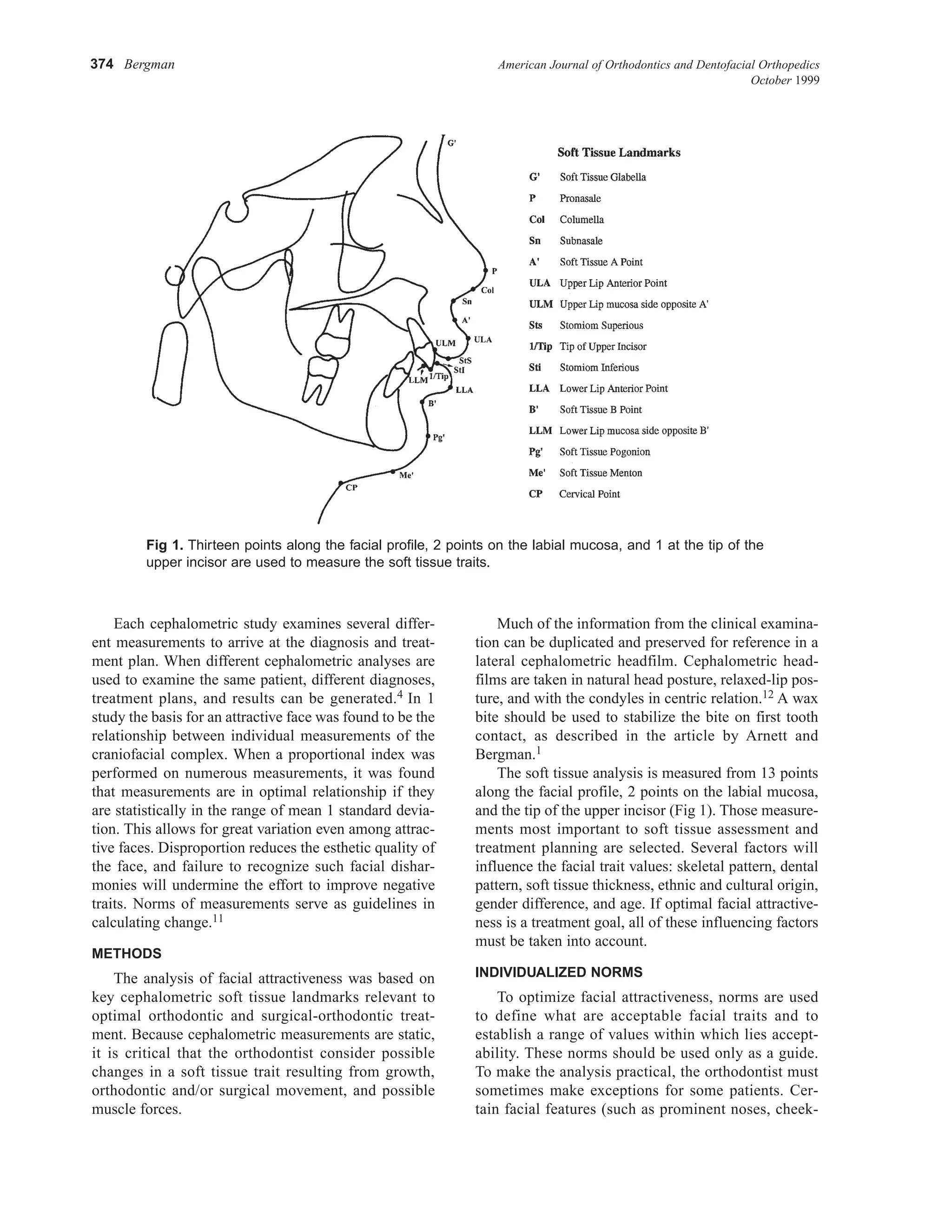
3) A thorough examination of 18 key soft tissue facial traits is necessary for treatment planning to optimize facial attractiveness while correcting the bite. Individual












































































![Soft tissue cephalometric analysis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/softtissuecephalometricanalysisautosaved-250708101220-a738d47e-thumbnail.jpg?width=640&height=640&fit=bounds)























