Downloaded 35 times

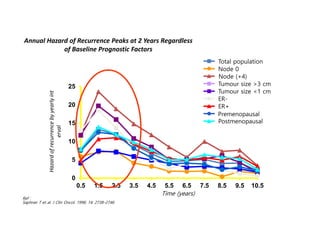

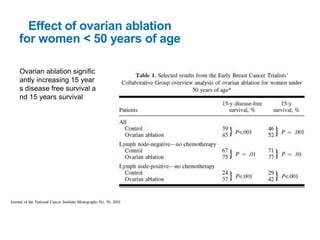
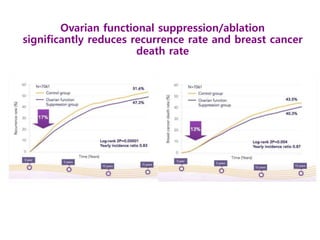
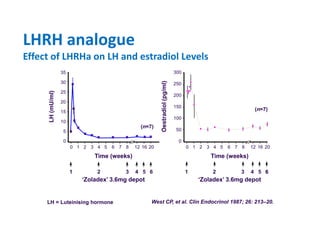
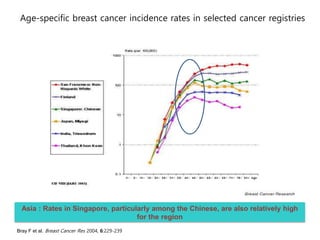
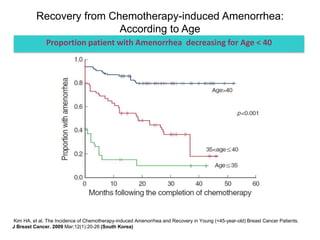
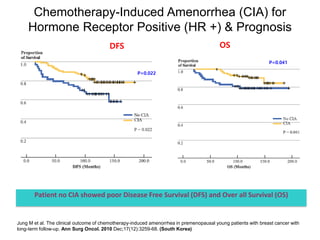

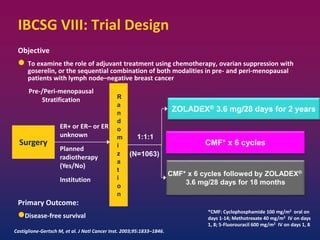
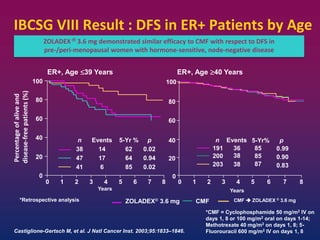
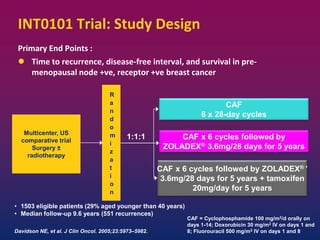
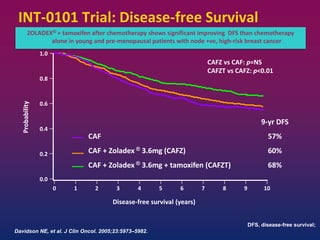
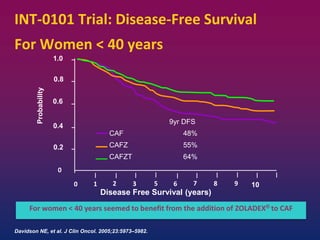
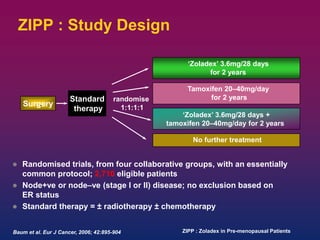
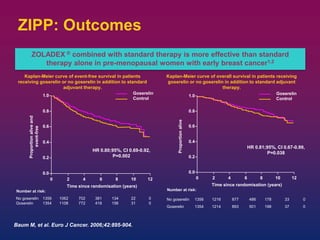
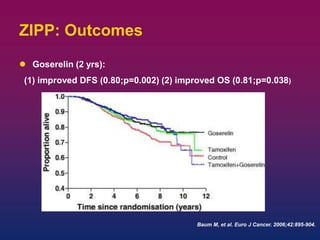

Breast cancer is the most common cancer in women worldwide, with an estimated 1.6 million new cases and over 500,000 deaths per year. A key document summarizes evidence from several studies showing that the addition of ovarian suppression/ablation through drugs like Zoladex to standard therapies improves outcomes for premenopausal breast cancer patients. Specifically, it improves disease-free survival when added to chemotherapy for young premenopausal patients. It also improves disease-free and overall survival when given for 2 years after chemotherapy compared to chemotherapy alone in high-risk premenopausal breast cancer patients.










































![metastaticbreastcancer-200622051104 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/metastaticbreastcancer-200622051104autosaved-250105083416-8390994c-thumbnail.jpg?width=640&height=640&fit=bounds)





![Hemorrhoid ambeyen hemorhoid azis[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hemorrhoidpantiwaluyo1-231013142359-b576a3e3-thumbnail.jpg?width=640&height=640&fit=bounds)