ara.roy1710@gmail.com
Cognitive Behavioural Therapy(CBT)
Beck (1960s)
“The stronger person is not the one making the
most noise but the one who can quietly direct
the conversation toward defining and solving
problems.”
Aaron Temkin Beck.
(1921-2021)
4.
ara.roy1710@gmail.com
Introduction.
• Initially developedin the early 1960s by Dr. Aaron Beck of the University of
Pennsylvania.
• During clients’ cognitive development they learn incorrect habits of
processing and interpreting information.
• Aim is thus to unravel these distortions and help them to learn more
different and realistic ways of processing and reality-testing information.
5.
ara.roy1710@gmail.com
Basic concepts.
• ‘Cognition’is defined as that function that involves inferences about
one’s experiences and about the occurrence and control of future
events. It includes the processes involved in identifying and predicting
complex relations among events for the purposes of adaptation.
• Humans have capacity for both primal/primitive and for higher level
cognitive processing.
6.
ara.roy1710@gmail.com
Basic concepts.
• Schemas.
Structuresthat consist of people’s fundamental beliefs and assumptions.
They are meaning making cognitive structures. They are relatively stable
cognitive patterns that influence through their beliefs, how people select and
synthesize incoming information. Developed early in life through personal
experiences and identification with significant others and reinforced by
further learning experiences.
7.
ara.roy1710@gmail.com
Basic concepts.
• Modes.
Networksof cognitive, affective, motivational and behavioural
schemas. Modes are fundamental to personality since they interpret
and adapt to emerging and ongoing situations. CBT approaches
dysfunctional modes by deactivating them, modifying their content
and structure and by constructing adaptive modes to neutralize them.
8.
ara.roy1710@gmail.com
Basic concepts.
• Cognitivevulnerability.
Refers to humans’ cognitive frailty. Because of their schemas, each
person has a set of unique vulnerabilities and sensitivities that
predispose them to psychological distress. When they exhibit
psychological problems, their dysfunctional schemas and beliefs lead
them systematically to bias information in unhelpful ways.
ara.roy1710@gmail.com
Basic concepts.
• Automaticthoughts.
Thoughts which occur spontaneously, without effort or choice. In
psychological disorders, automatic thoughts are often distorted, extreme, or
otherwise inaccurate.
Not so deeply buried as beliefs and schemas. People’s self-evaluations and
self-instructions appear to be derived from deeper structures- their self-
schemas (deeper beliefs and assumptions).
ara.roy1710@gmail.com
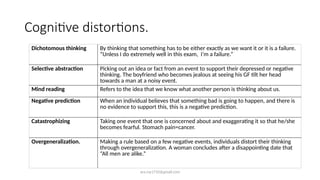
Cognitive distortions.
Dichotomous thinkingBy thinking that something has to be either exactly as we want it or it is a failure.
“Unless I do extremely well in this exam, I’m a failure.”
Selective abstraction Picking out an idea or fact from an event to support their depressed or negative
thinking. The boyfriend who becomes jealous at seeing his GF tilt her head
towards a man at a noisy event.
Mind reading Refers to the idea that we know what another person is thinking about us.
Negative prediction When an individual believes that something bad is going to happen, and there is
no evidence to support this, this is a negative prediction.
Catastrophizing Taking one event that one is concerned about and exaggerating it so that he/she
becomes fearful. Stomach pain=cancer.
Overgeneralization. Making a rule based on a few negative events, individuals distort their thinking
through overgeneralization. A woman concludes after a disappointing date that
“All men are alike.”
13.
ara.roy1710@gmail.com
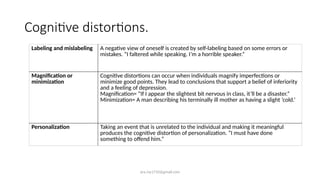
Cognitive distortions.
Labeling andmislabeling A negative view of oneself is created by self-labeling based on some errors or
mistakes. “I faltered while speaking. I’m a horrible speaker.”
Magnification or
minimization
Cognitive distortions can occur when individuals magnify imperfections or
minimize good points. They lead to conclusions that support a belief of inferiority
and a feeling of depression.
Magnification= “If I appear the slightest bit nervous in class, it’ll be a disaster.”
Minimization= A man describing his terminally ill mother as having a slight ‘cold.’
Personalization Taking an event that is unrelated to the individual and making it meaningful
produces the cognitive distortion of personalization. “I must have done
something to offend him.”
14.
ara.roy1710@gmail.com
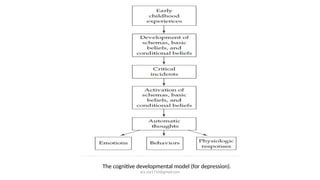
Cognitive model ofdevelopment of schemas.
• Individual beliefs begin in early childhood and develop throughout life. Early
childhood experiences lead to basic beliefs about oneself and one’s world.
• These beliefs can be organized into cognitive schemas.
• Positive experiences of support and love from parents, lead to beliefs such
as “I am lovable” and “I am competent,” which in turn lead to positive
views/cognitive schemas of themselves in adulthood.
15.
ara.roy1710@gmail.com
Cognitive model ofdevelopment of schemas.
• Persons who develop psychological dysfunctions, in contrast to those with healthy functioning, have
negative experiences that may lead to beliefs such as “I am unlovable” and “I am inadequate.”
• These developmental experiences, along with critical incidents/traumatic experiences, influence
individuals’ belief systems.
• Negative experiences, such as being ridiculed by someone, may lead to conditional beliefs such as “If
others don’t like what I do, I am not valuable.”
• Such beliefs may become basic to the individual as negative/maladaptive cognitive schemas.
16.
ara.roy1710@gmail.com
Cognitive model ofdevelopment of schemas.
• Early maladaptive schemas.
Assumed to be true about themselves and their world.
Resistant to change
Cause difficulties in individual’s lives.
Usually activated by a change in one’s world (triggering event), such as
a loss of a job.
17.
ara.roy1710@gmail.com
Cognitive model ofdevelopment of schemas.
When these conditions occur, individuals often react with strong negative
emotions.
Are the result of previous dysfunctional childhood interactions with family
members.
Through these belief systems that children develop, they start to view reality in
ways that cause problems in functioning internally or with others.
Likely to continue through adolescence and adulthood.
ara.roy1710@gmail.com
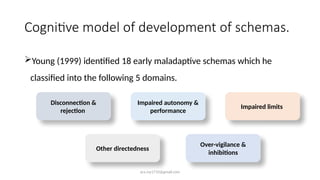
Cognitive model ofdevelopment of schemas.
Young (1999) identified 18 early maladaptive schemas which he
classified into the following 5 domains.
Disconnection &
rejection
Impaired autonomy &
performance
Impaired limits
Over-vigilance &
inhibitions
Other directedness
25.
ara.roy1710@gmail.com
Goals of therapy.
Identifyingnegative automatic thoughts (NATs) and the cognitive
schemas that they represent.
Changing the dysfunctional cognitive schemas through:
Schema
reinterpretatio
n
Schema
modification
Schema
restructuring
26.
ara.roy1710@gmail.com
Goals of therapy.
Toremove biases or distortions in thinking so that individuals may
function more effectively.
• NOTE: Generally, when establishing goals, cognitive therapists focus on
being specific, prioritizing goals, and working collaboratively with clients.
The goals may have affective, behavioral, and cognitive components.
27.
ara.roy1710@gmail.com
Assessment in CBT.
•Careful attention is paid to
assessment of client problems and
cognitions, both at the beginning
of therapy and throughout the
entire process, so that the therapist
may clearly conceptualize and
diagnose the client’s problems.
• client interviews
• self-monitoring
• thought sampling,
• assessment of beliefs and
assumptions
• self-report questionnaires
Techniques.
28.
ara.roy1710@gmail.com
Therapeutic process.
• Structuredin approach.
Initial phase:
assessment of the problem
development of collaborative therapeutic
relationship
Case conceptualization
Middle phase:
helping client identify/learn about his
inaccurate thinking
identifying NATs
Guided discovery approach employed;
Homework assigned.
Termination phase:
insight developing
implementing learned strategies
moving towards change.
29.
ara.roy1710@gmail.com
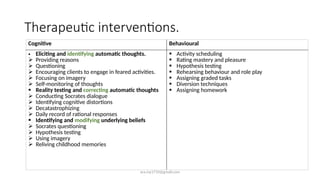
Therapeutic interventions.
Cognitive Behavioural
•Eliciting and identifying automatic thoughts.
Providing reasons
Questioning
Encouraging clients to engage in feared activities.
Focusing on imagery
Self-monitoring of thoughts
Reality testing and correcting automatic thoughts
Conducting Socrates dialogue
Identifying cognitive distortions
Decatastrophizing
Daily record of rational responses
Identifying and modifying underlying beliefs
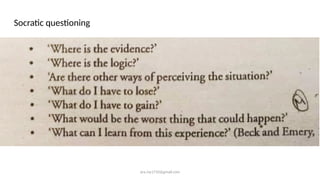
Socrates questioning
Hypothesis testing
Using imagery
Reliving childhood memories
Activity scheduling
Rating mastery and pleasure
Hypothesis testing
Rehearsing behaviour and role play
Assigning graded tasks
Diversion techniques
Assigning homework
#3 AB born. 1921. Third surviving son of Russian Jewish immigrant parents. Parents had an elder son before and an only daughter to influenza in 1919 leading AB’s mother into a period of depression (episodes present throughout life).
At 7 years of age, Beck had a near-fatal disease which reinforced his mother’s overprotectiveness. Beck came to think that he was a replacement for his sister, and that his mother was disappointed that he was not a girl. When Beck was seven years old, he broke an arm in a playground accident. The broken bone became infected, resulting in a generalized septicemia (blood poisoning) that kept him in the hospital long enough to miss promotion into second grade.
Beck missed his friends and didn't like being a grade behind them. With the help of some tutoring from his older brothers, as well as his own determination, Beck not only caught up with his former classmates but ended up being promoted a year ahead of them. He regarded his success as a psychological turning point.
Developed phobias while growing up: blood/injury phobia, which he related to his experience with surgery for his broken arm at age seven. The surgeon apparently began to make the incision before Beck was fully anesthetized.
Fear of suffocation, which was apparently caused by a bad case of whooping cough, chronic childhood asthma, and an older brother who used to tease Beck by putting a pillow over his face.
Fears of heights and of public speaking. Beck also drew from his own experiences when writing his first book on depression, which he published in 1967 (The diagnosis and management of depression) . Beck was mildly depressed while he was writing the book, but regarded the project as a kind of self-treatment.
#4 Beck's cognitive therapy may be categorized as a variant of constructivism.
Posits that humans are meaning-makers in their lives and essentially construct their own realities.
Actively engaged in ordering their experiences through assigning emotional as well as intellectual significance to them.
Determine their own life course.
Humans continue to grow and develop over the entire course of their lifespan.
#6 Schemas are NOT pathological by definition. They can be ‘adaptive’ or ‘maladaptive.’ They can range from being ‘latent’ to ‘predominant.’ When they are ‘hypervalent’ they are pre-potent and easily triggered.
Psychopathology= crowding of maladaptive schemas + Inhibition of adaptive schemas.
#8 Childhood traumas (a 5-year old who went away on a trip and returned to find the family dog dead, develops the belief, “When I’m physically not close to others, something bad will happen.”)
Negative treatment in childhood (negative parenting/abuse)
Social learning/ modelling (marital partners have memories about how parents behaved; parent modelling may thus provide the rules and regulations, shoulds and should-nots that the couple brings into the marriage.
Inadequate experiences for the learning of coping skills
#10 They are less accessible to awareness than voluntary thoughts.
Counterpart of what Freud called “preconscious thinking.”
They are part of a person’s internal monologue- can take the form of both words and images.
#12 Dysfunctional beliefs embedded in cognitive schemas contribute to systematic cognitive distortions, more accessible in automatic thoughts, that both characterise and maintain psychological distress.
#29 Therapists can provide reasons for the importance of examining the connections between how clients think, feel and act. Furthermore they can introduce the concept of NATs and provide an example of how underlying perceptions influence feelings.

















![Anxiety disorders unit intervention[2]](https://cdn.slidesharecdn.com/ss_thumbnails/anxietydisordersunitintervention2-111028091300-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






































