Downloaded 332 times

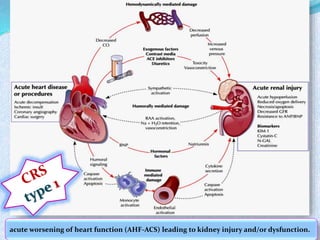
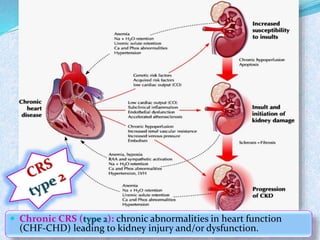
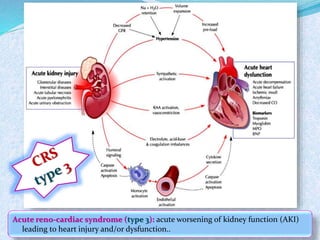
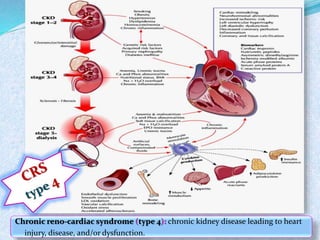
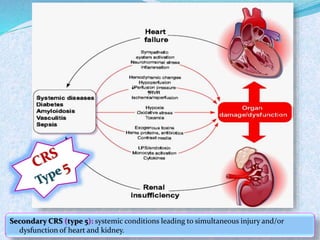
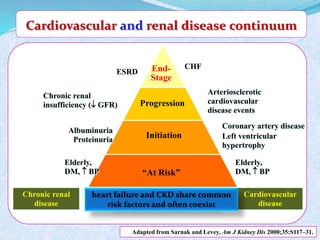

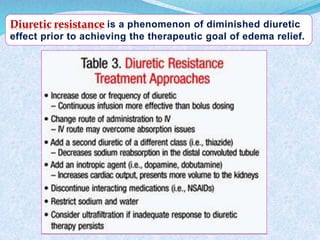


1. Cardio-renal syndrome (CRS) describes conditions where acute or chronic dysfunction in one organ induces acute or chronic dysfunction in the other organ. 2. Management of CRS is challenging and involves diuretics, ACE inhibitors, beta blockers, and dialysis. However, treatment outcomes remain poor, with high mortality and rates of rehospitalization. 3. While advances have been made, CRS continues to significantly impact morbidity and mortality. Early multidisciplinary management may help improve outcomes, but effective new therapies are still needed to better treat and prevent this challenging condition.













































































