Download as PDF, PPTX
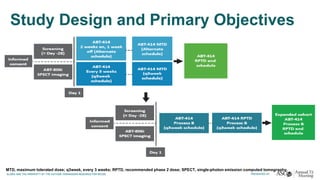
![Adverse drug reactions
Incidence (%) of all grades of ADRs in ≥10% subjects [N= 76]
No grade 4 or 5 ADRs
Events All grades Grade 3
Diarrhea 57 (75) 9 (12)
Rash 36 (47) 0
Nausea 27 (36) 2 (3)
Fatigue 23 (30) 2 (3)
Vomiting 22 (29) 1 (1)
Bilirubin ↑ 21 (28) 5 (7)
Appetite ↓ 20 (26) 1 (1)
Anemia 9 (12) 3 (4)
2 out of 76 patients (2.6%) withdrawn due to treatment-related AEs
Blood bilirubin increased (G3)
Nausea, Vomiting (G3)
Similar to
erlotinib/lapatinib](https://image.slidesharecdn.com/carbonedtdiscussion-share-150713203745-lva1-app6892/85/Novel-Strategies-for-Attacking-the-Epidermal-Growth-Factor-Receptor-16-320.jpg)
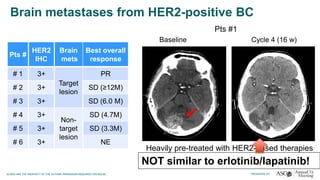

The document discusses innovative strategies for targeting the epidermal growth factor receptor (EGFR) in cancer treatment, particularly focusing on clinical trials for various combinations of inhibitors in EGFR-mutant lung cancer and other solid tumors. It details the results of several phase I trials, highlighting the efficacy and tolerability of new agents like S-222611 and ABT-414. The ongoing research aims to enhance treatment outcomes by addressing resistance mechanisms and optimizing drug combinations for improved patient response.























































































