Download to read offline











![Anatomical considerations
• Narrow stalk.
• Ascends out of the posterior cranial fossa through
the relatively small rigid opening in the tentorium
cerebelli.
• Two important cranial nerve nuclei.
• Reflex centers (the colliculi)
• the red nucleus and substantia nigra, [influencing
motor function]
• Ascending and descending tracts](https://image.slidesharecdn.com/brainstem-191117071504/75/Brain-stem-18-2048.jpg)
















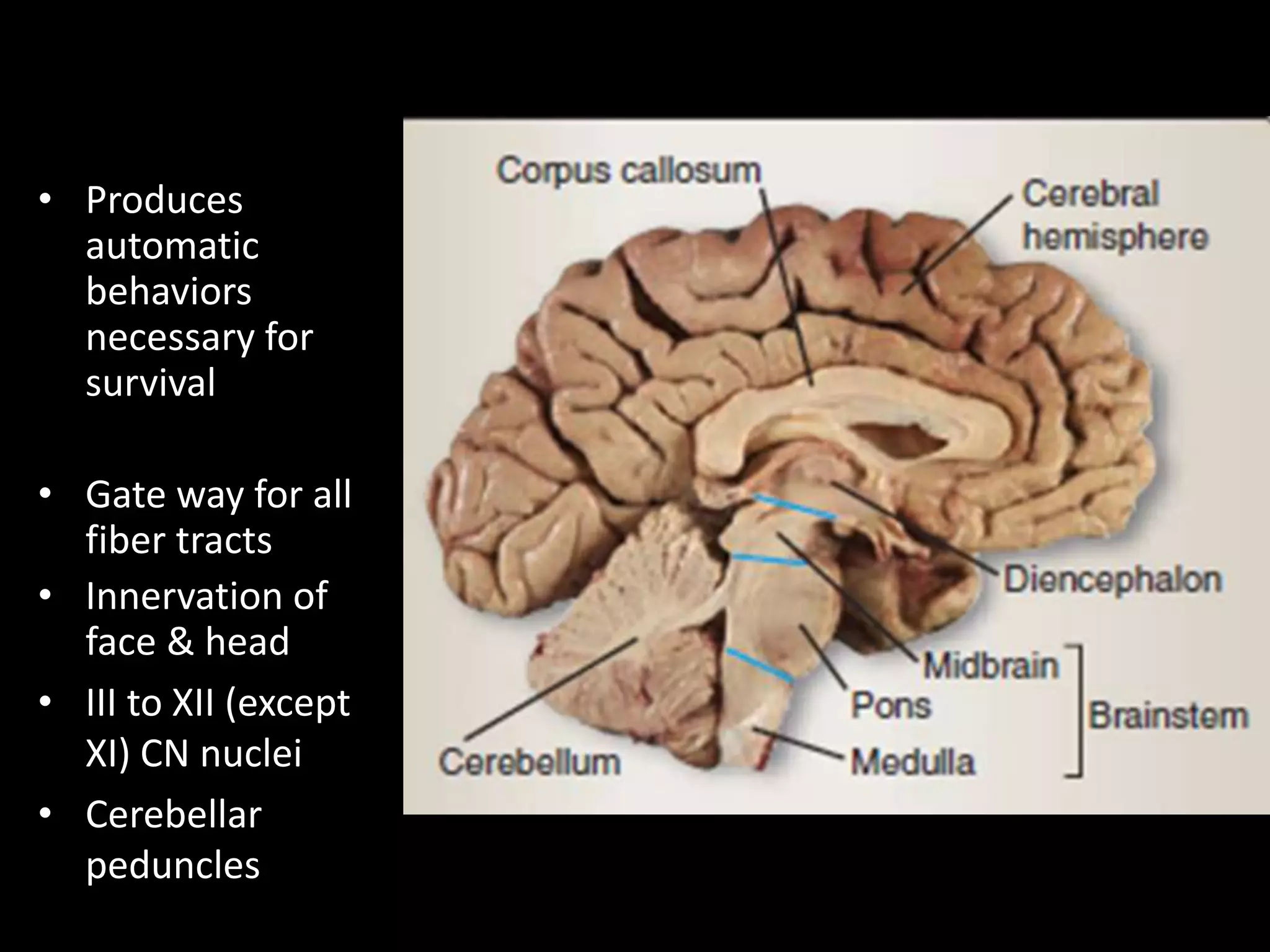
The document provides an overview of the brain stem, which is divided into 3 main sections - the midbrain, pons, and medulla. It describes the anatomical structures and nuclei contained within each section. Key functions include automatic behaviors for survival, relay of fiber tracts between the brain and spinal cord, and housing cranial nerve nuclei III-XII. The clinical significance is also summarized, outlining various neurological deficits that can result from lesions or vascular accidents affecting different parts of the brain stem.



































































