Download as PPSX, PPTX



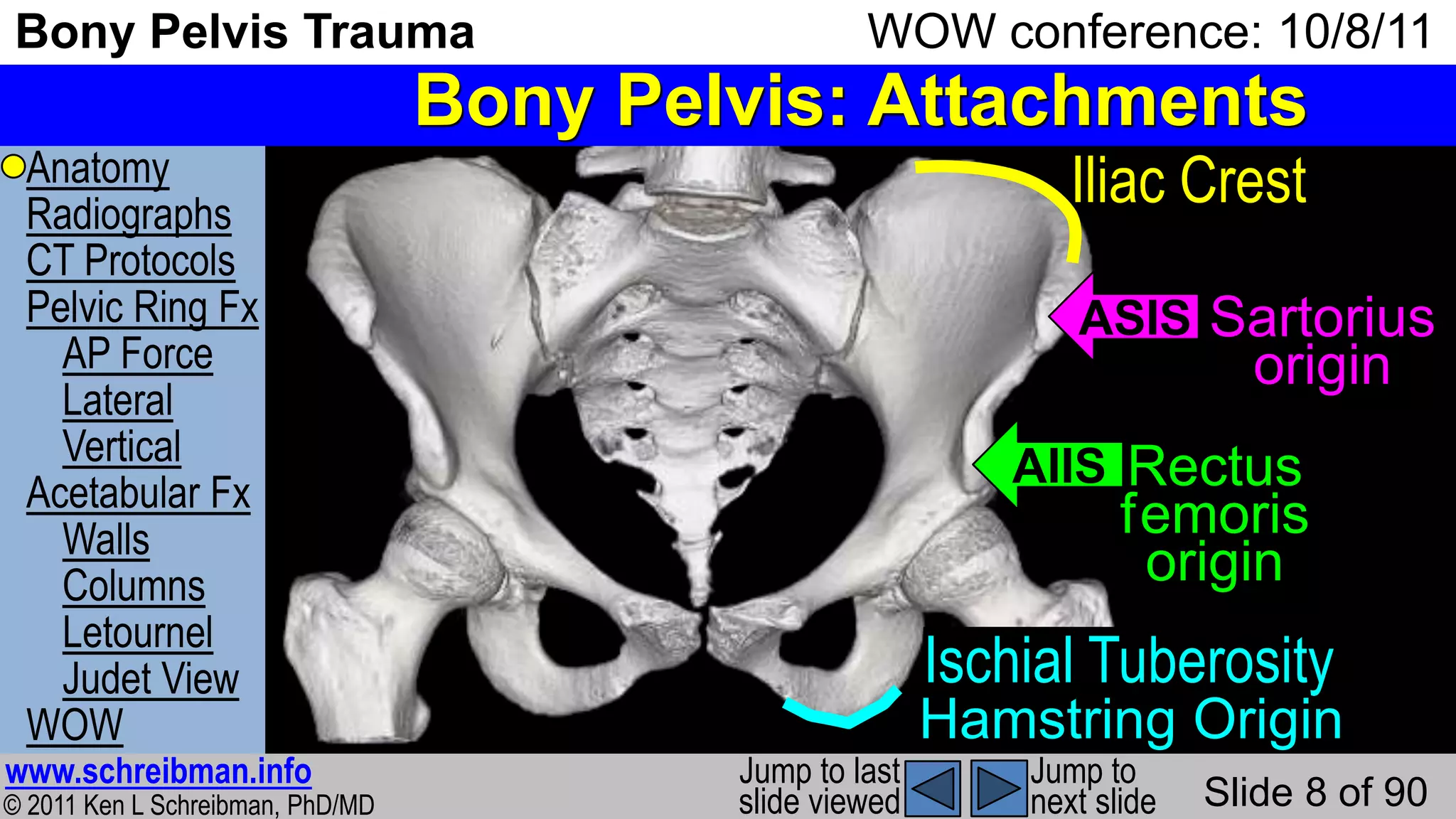
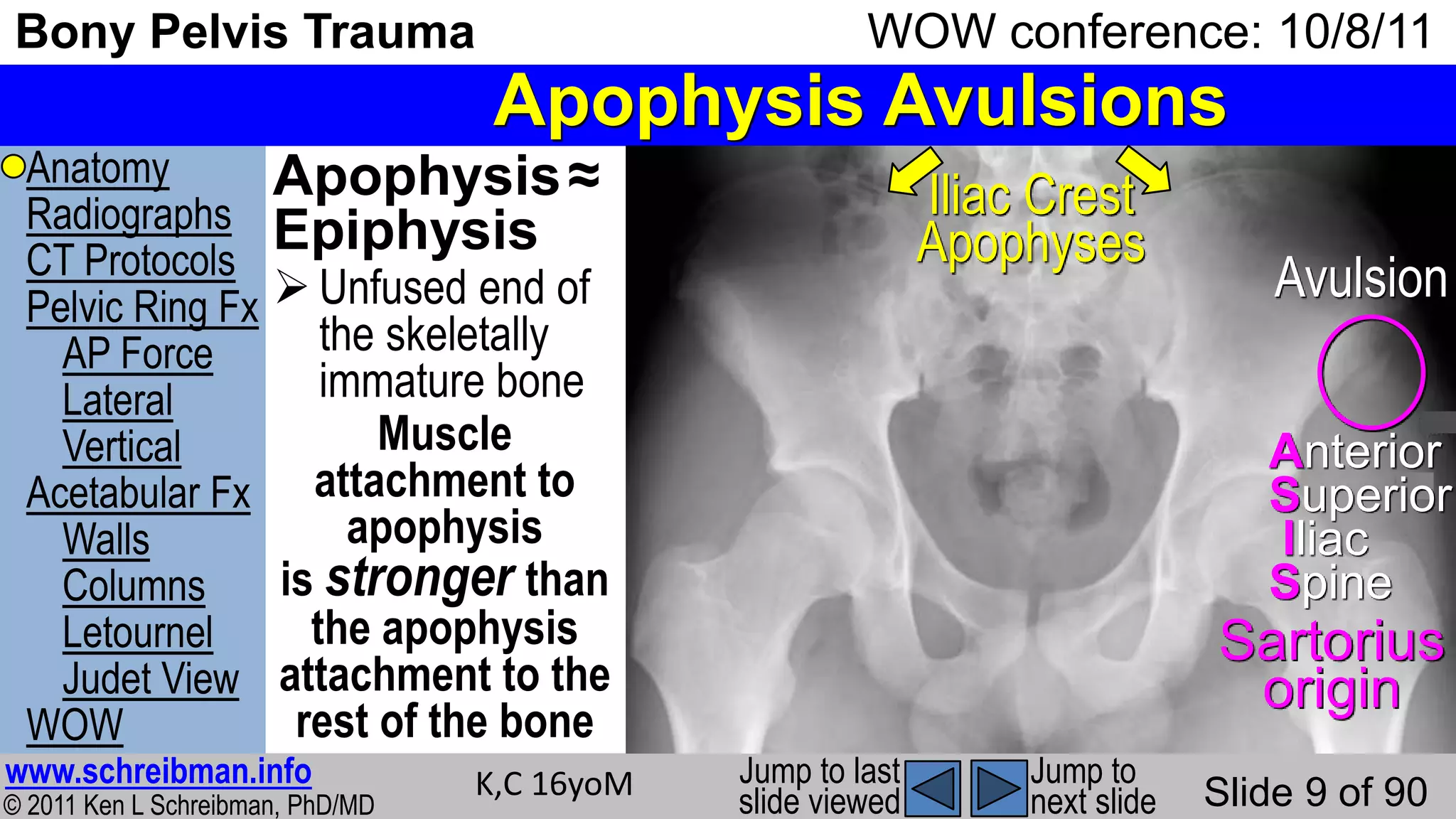
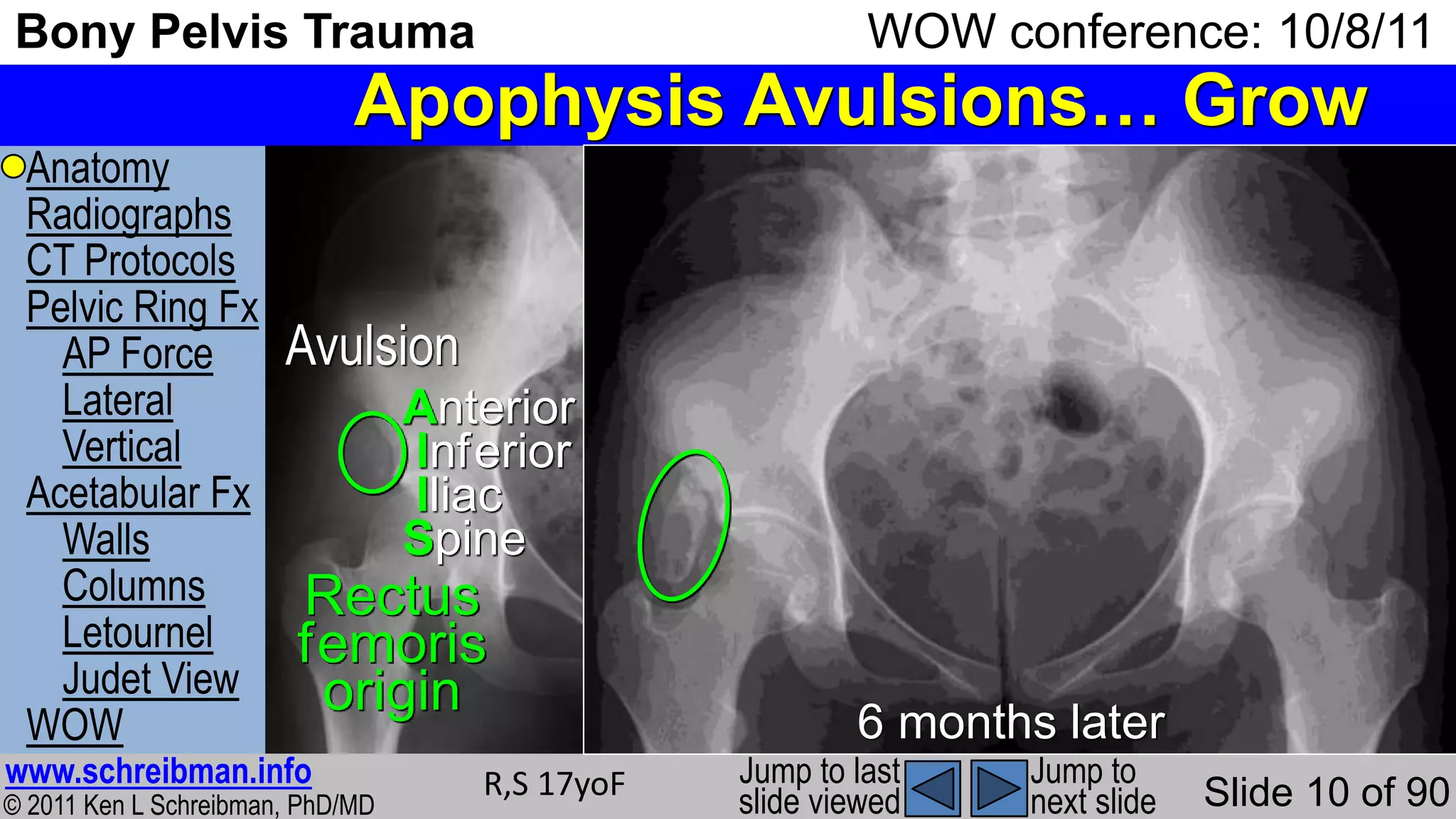
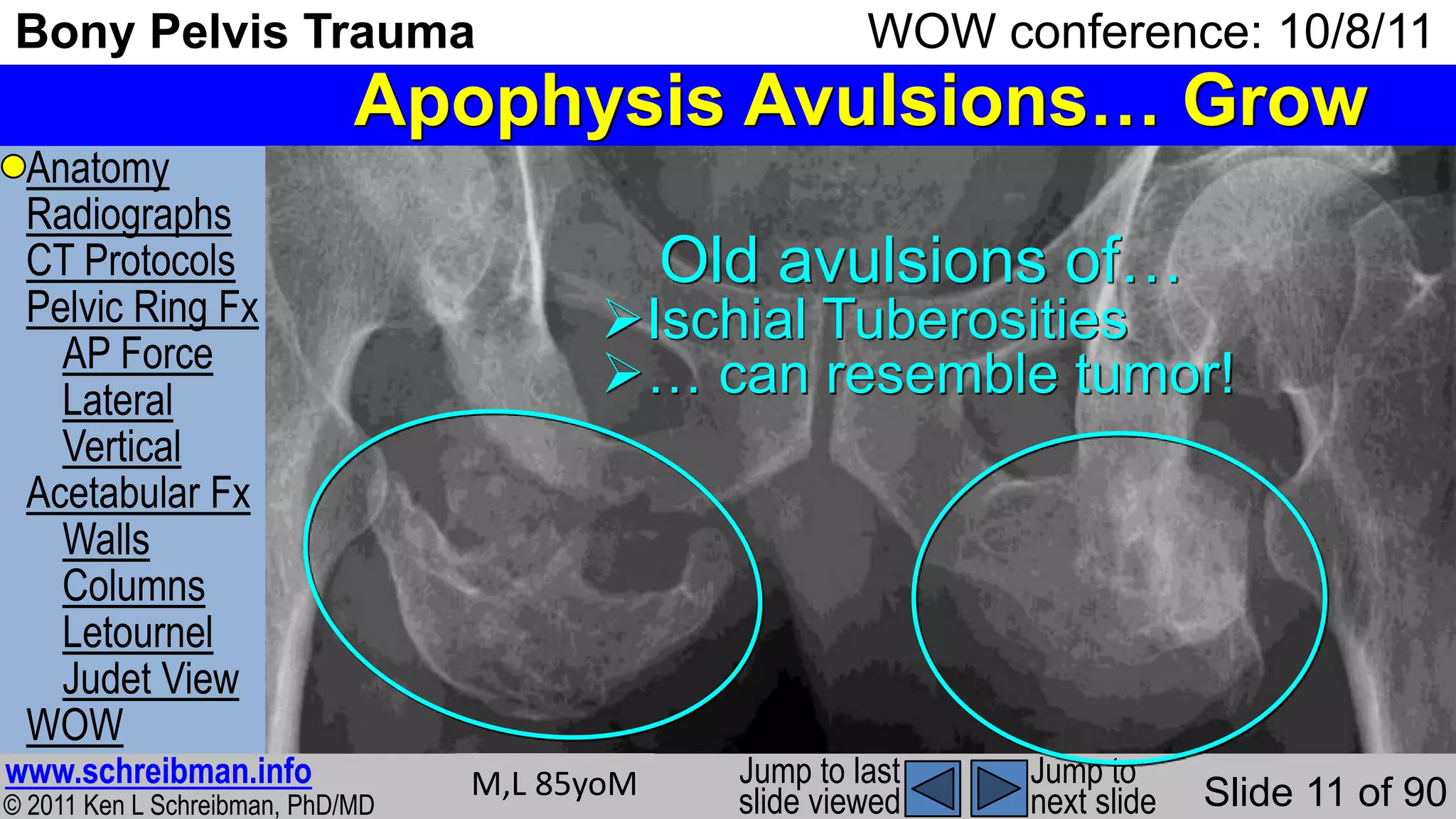



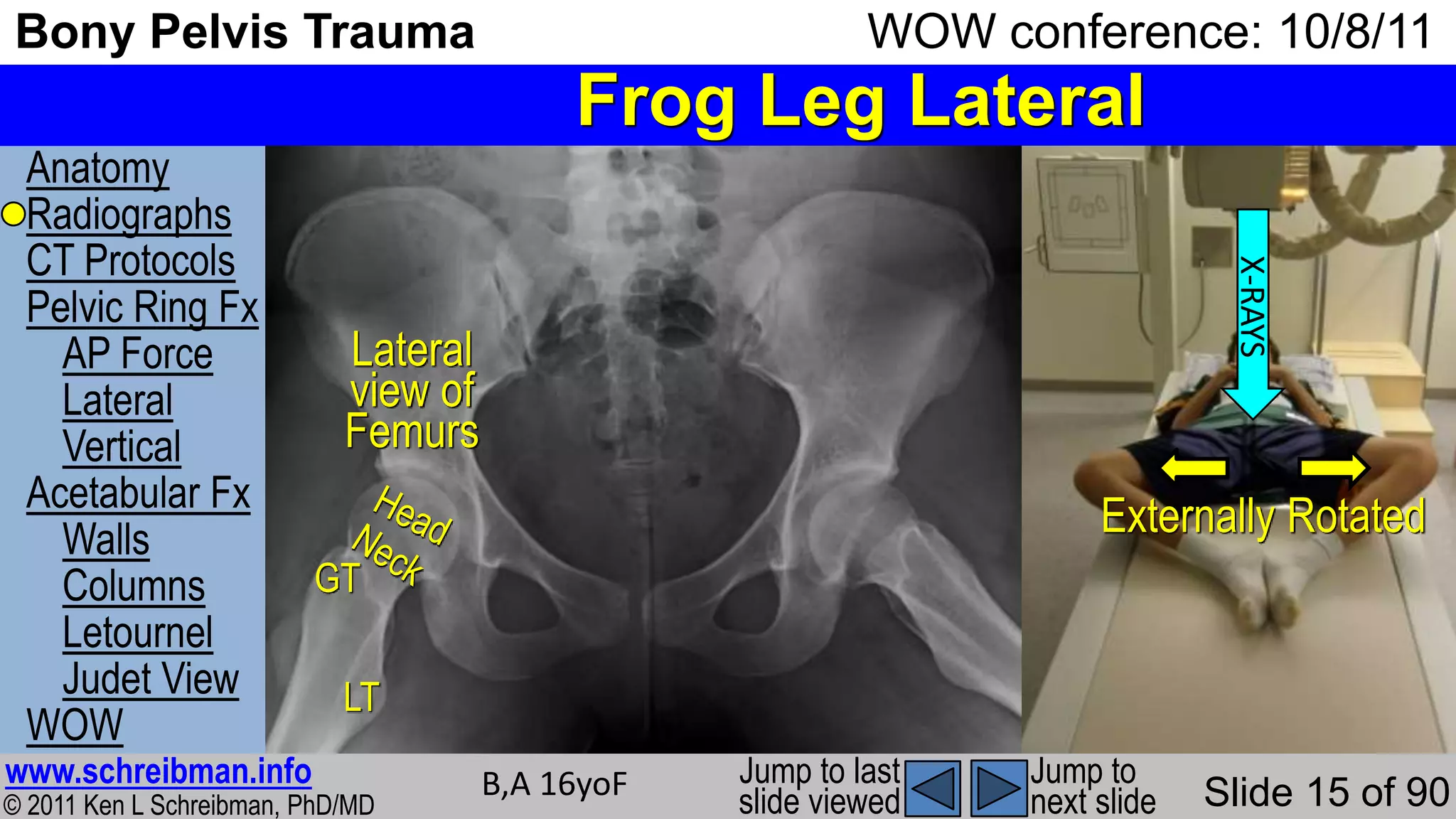
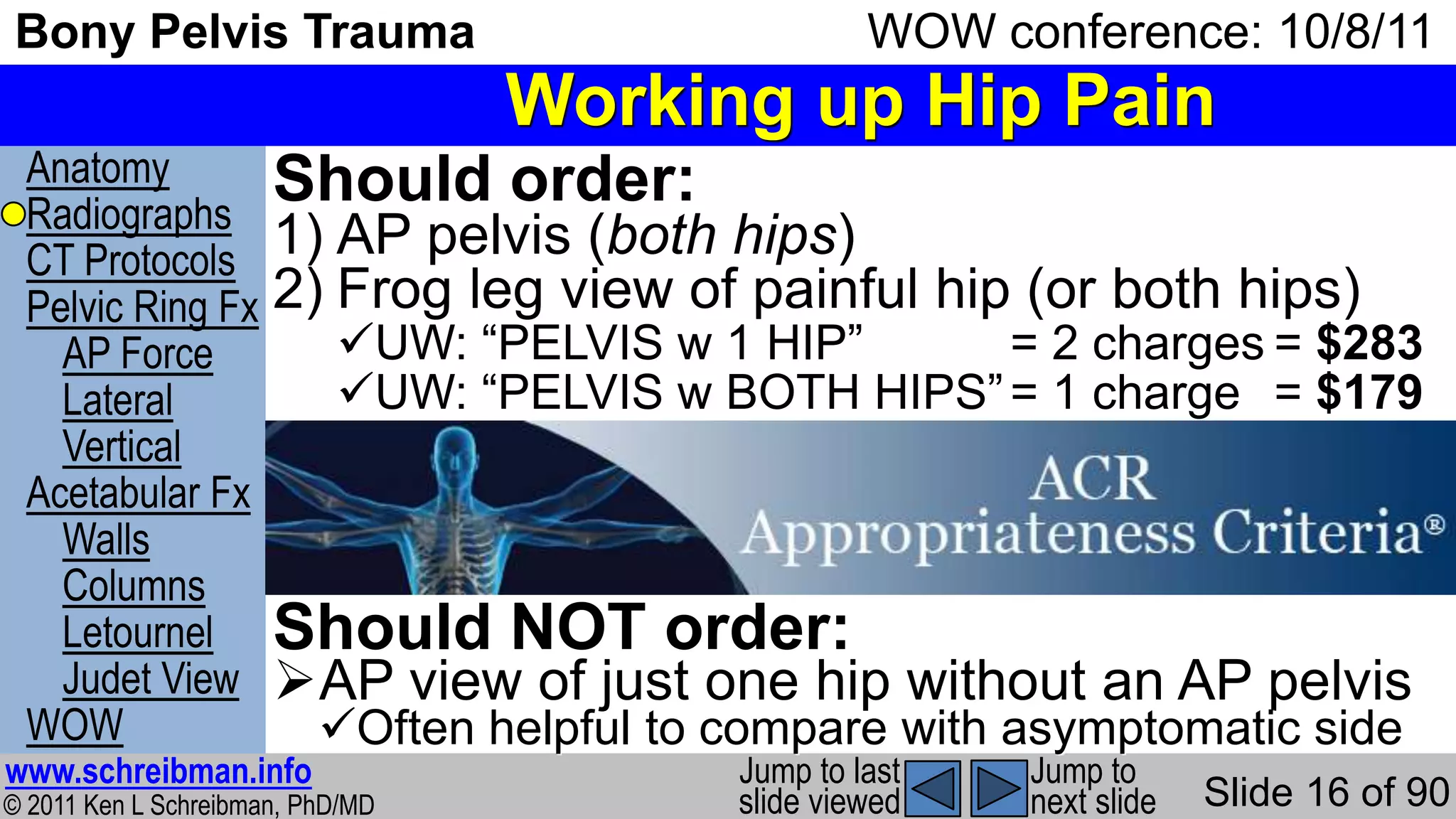


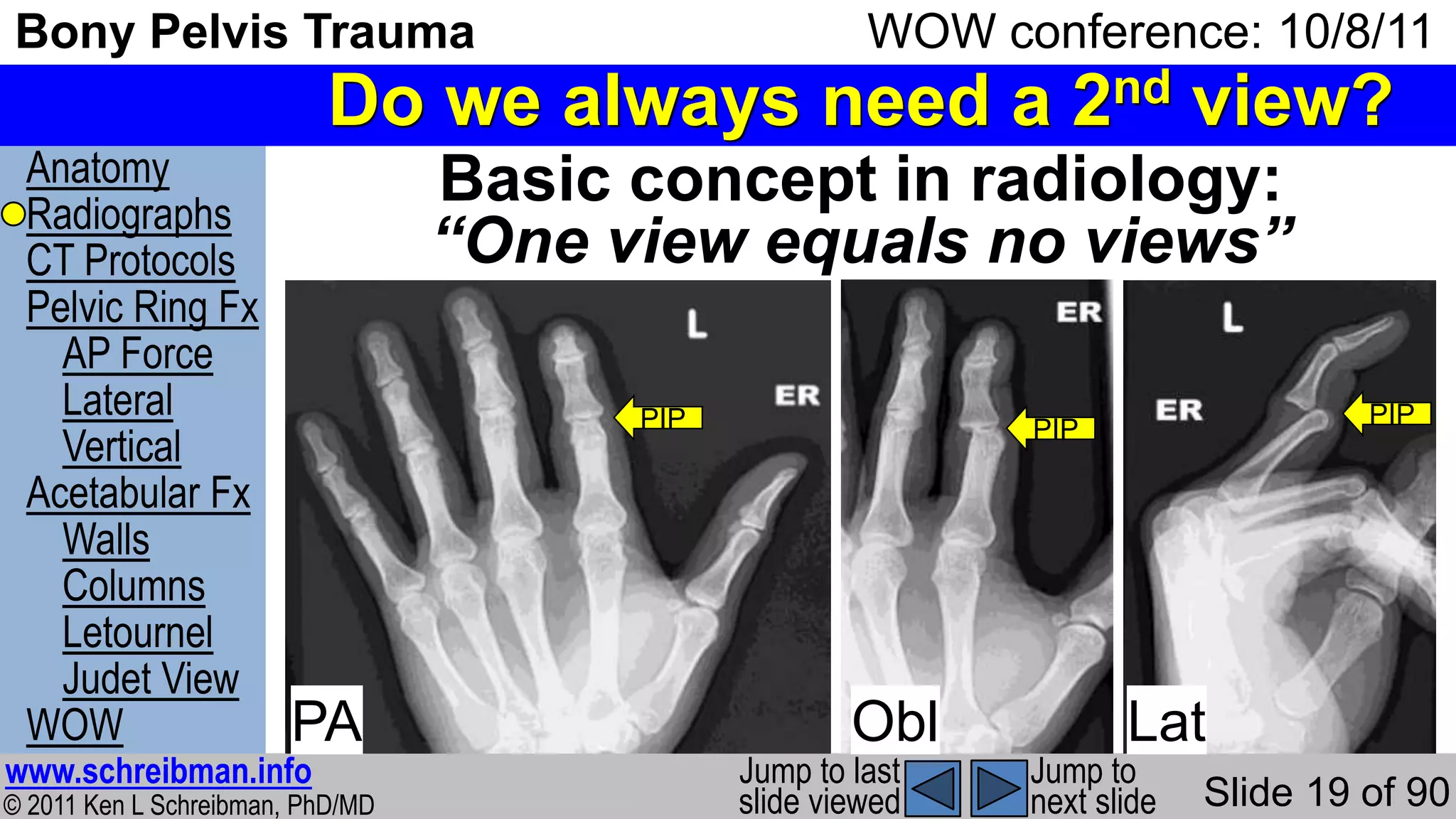

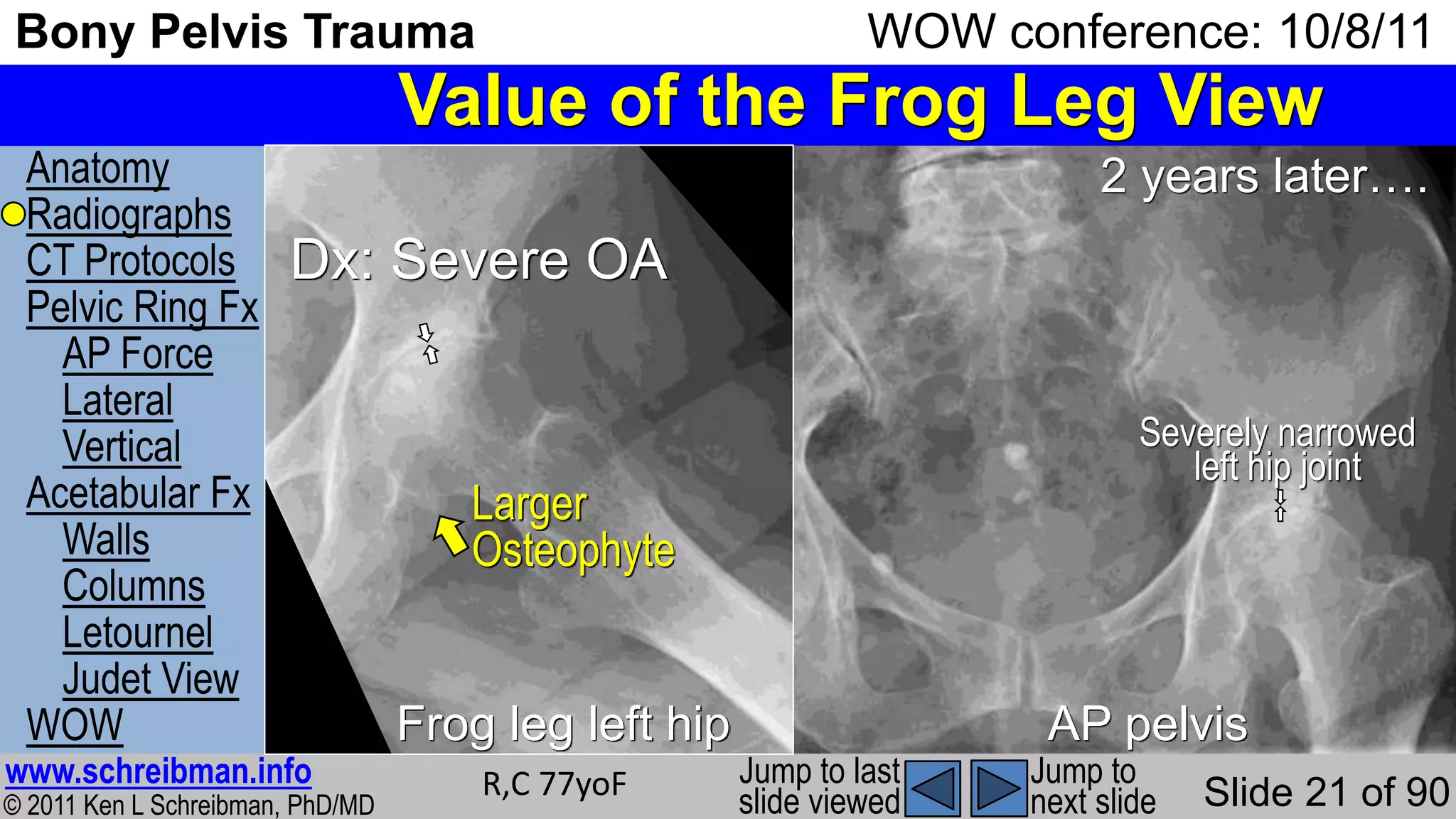

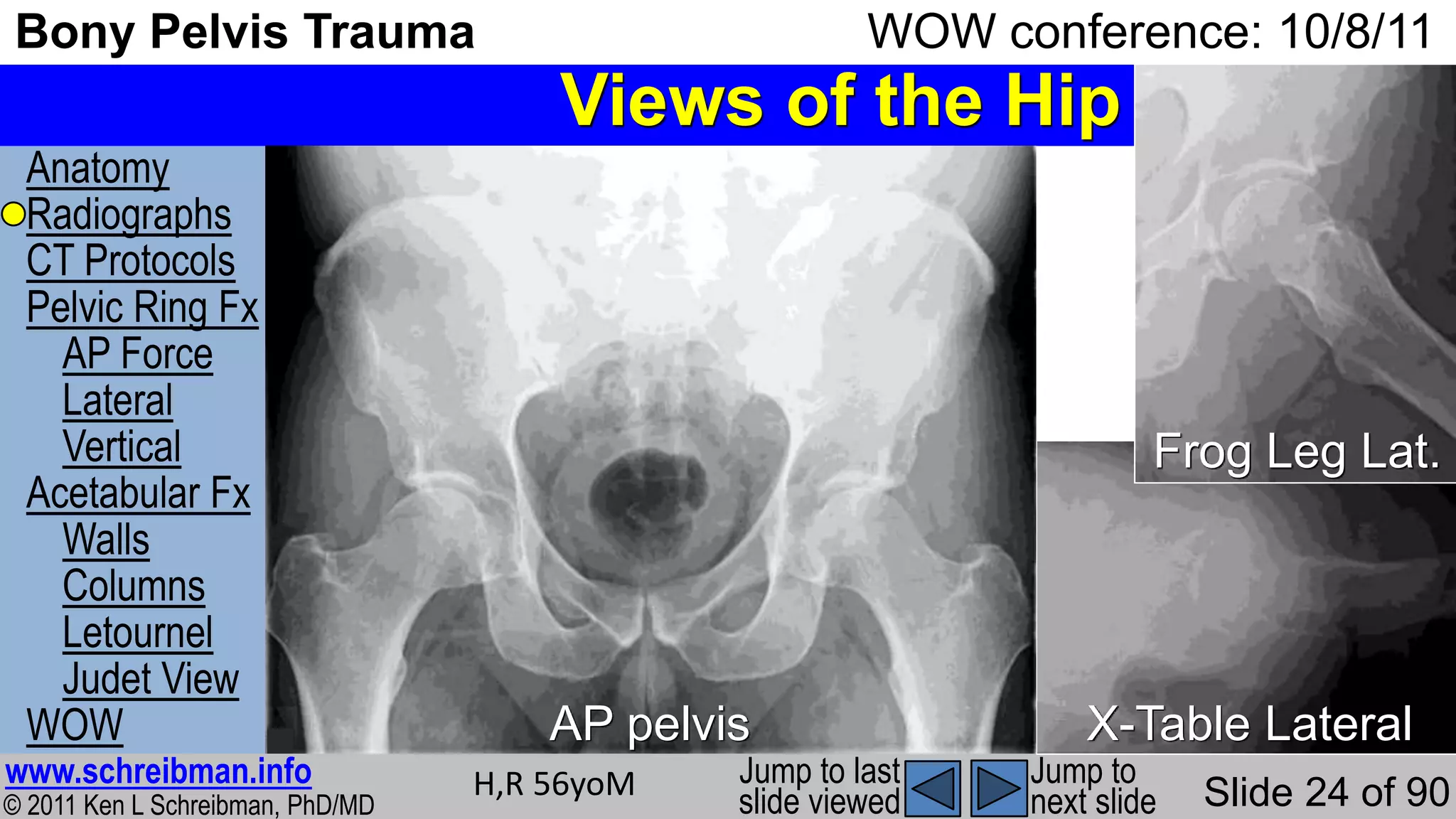

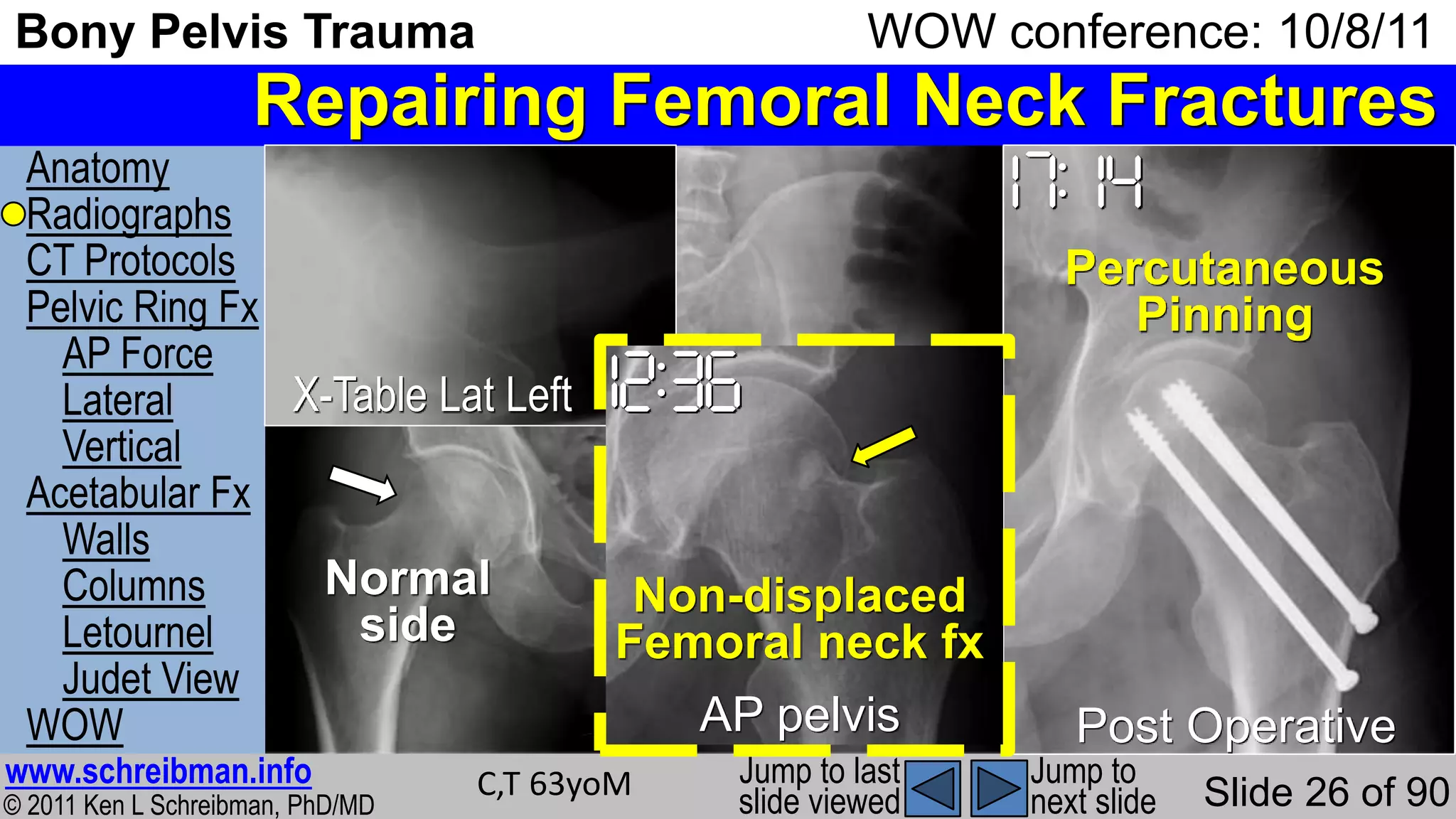



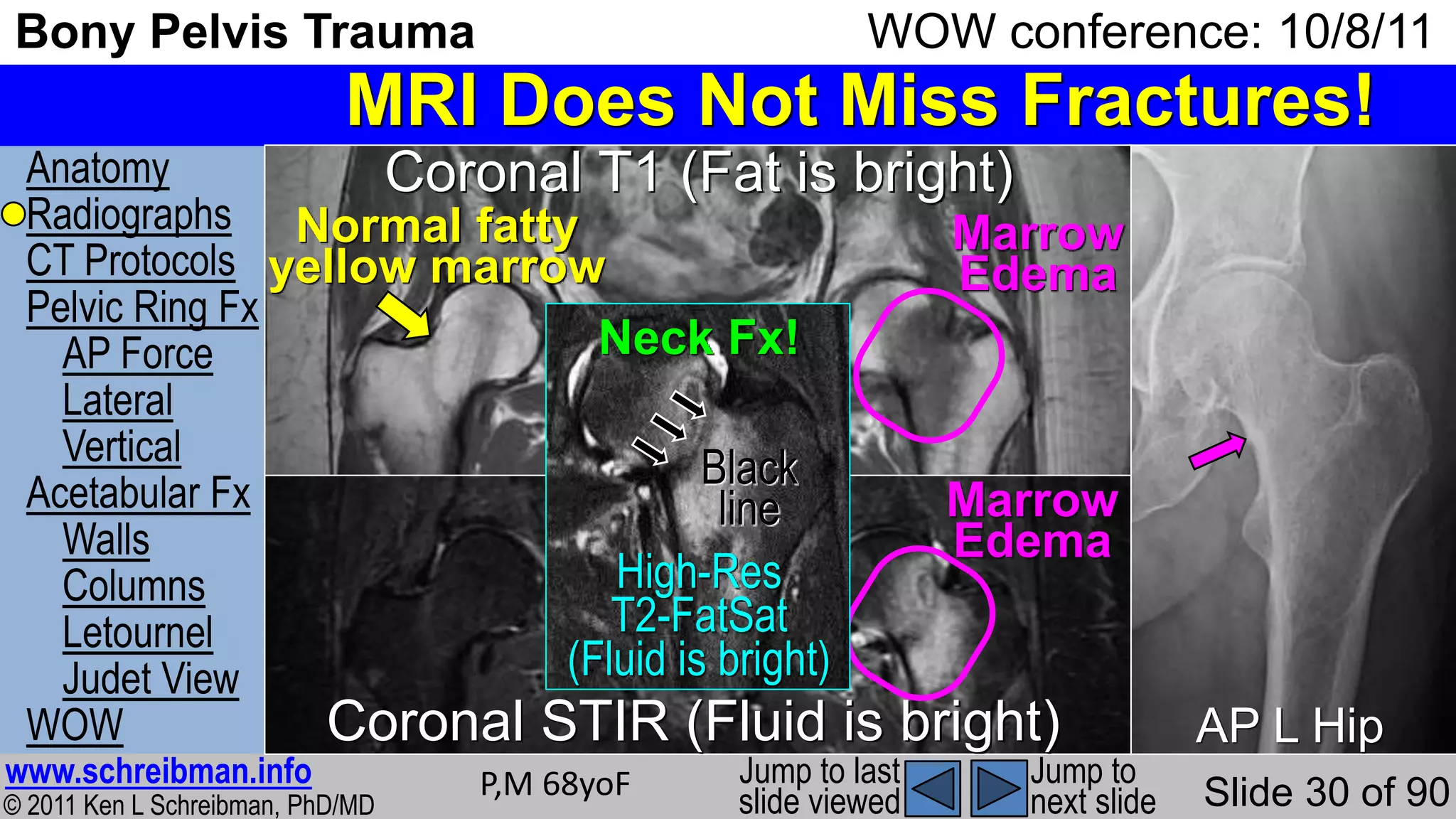


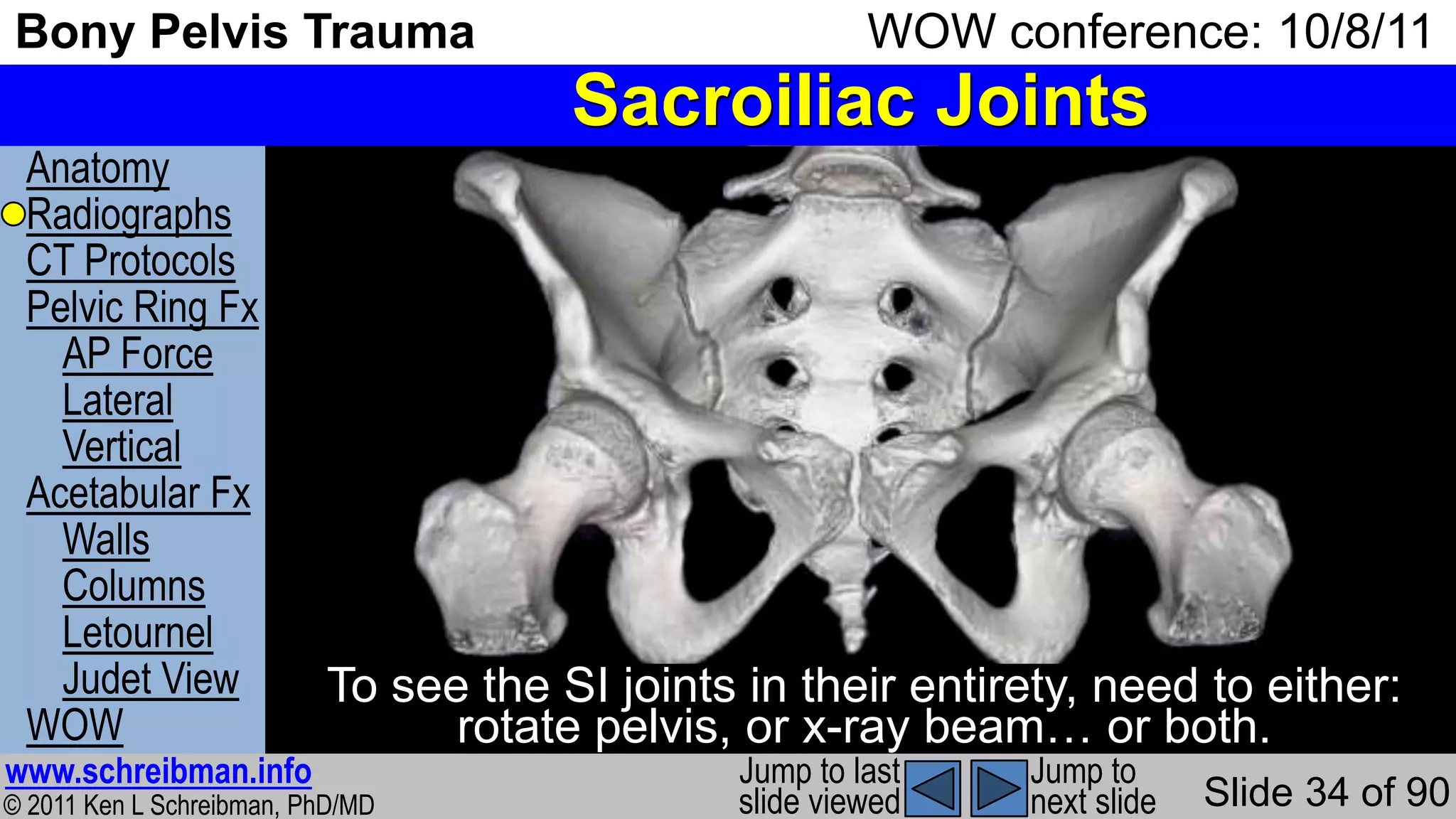
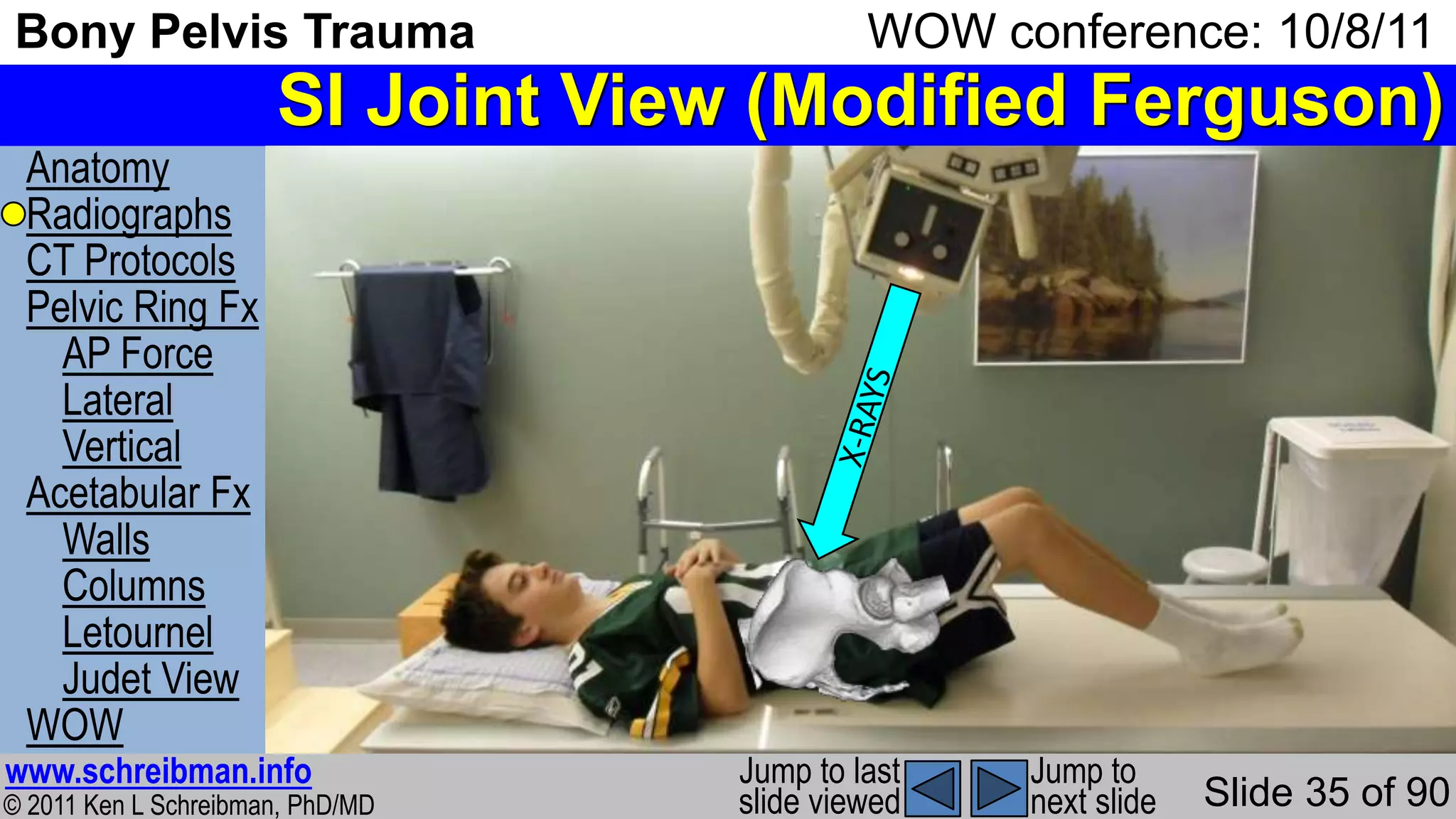





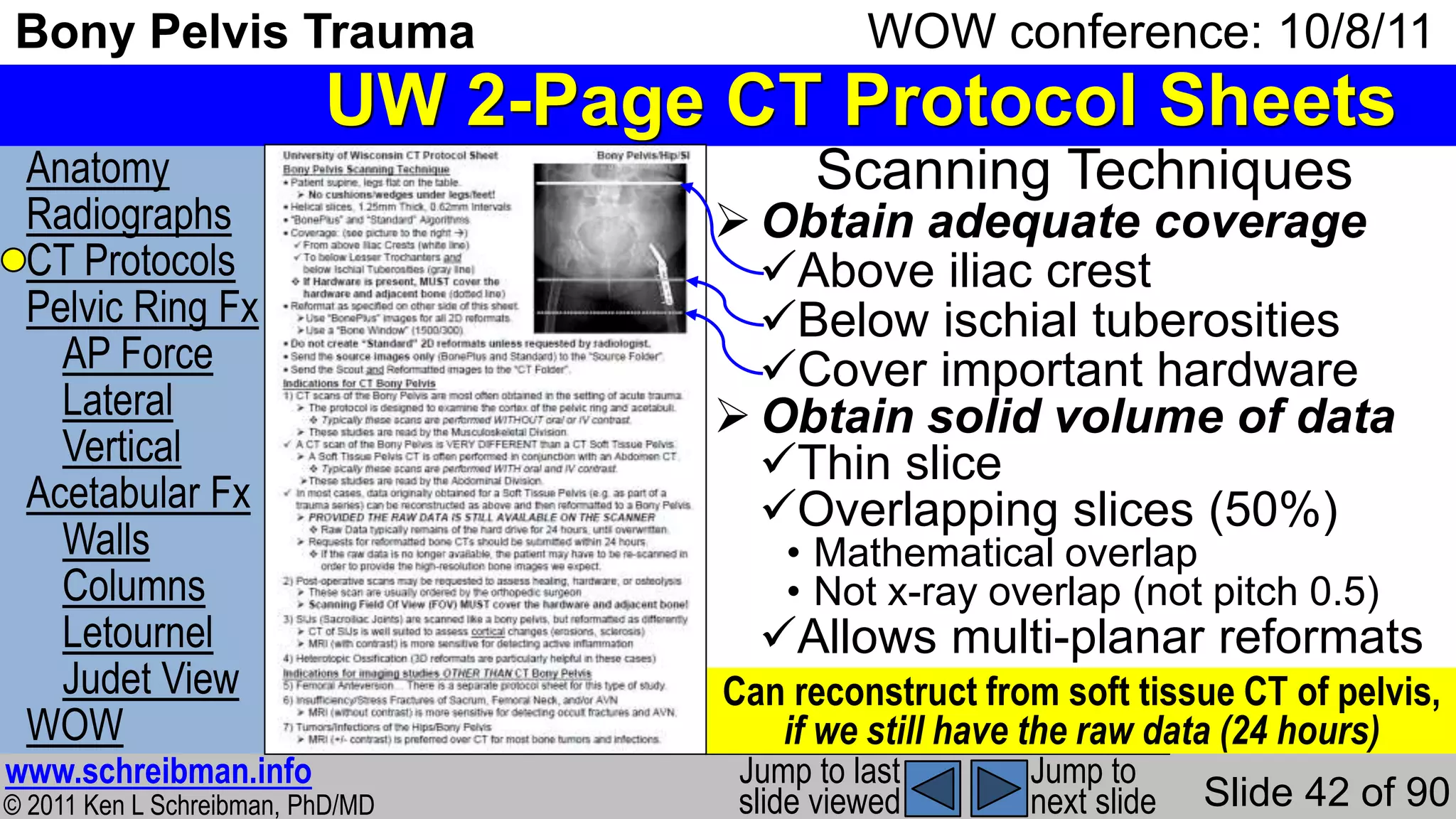
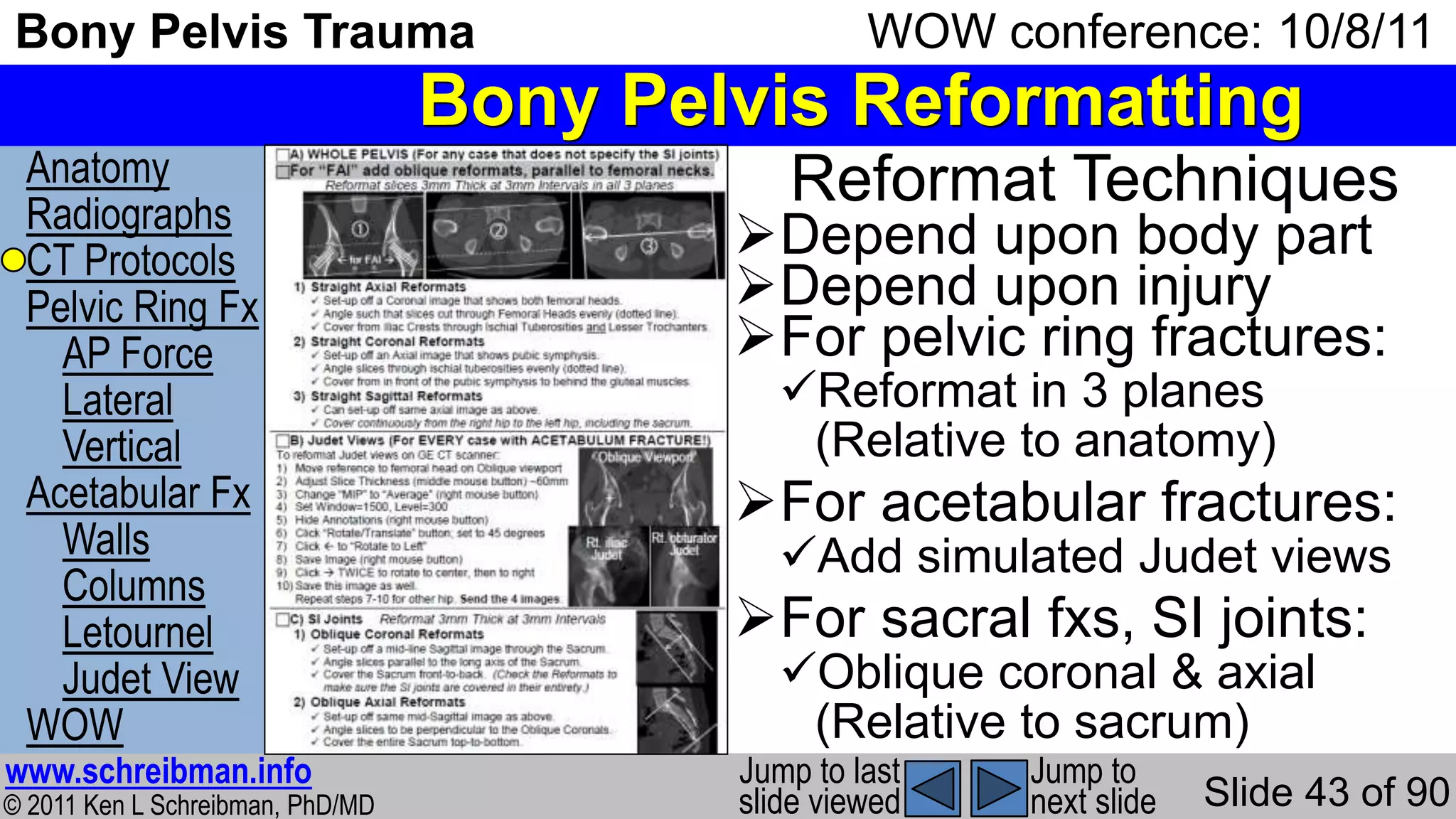
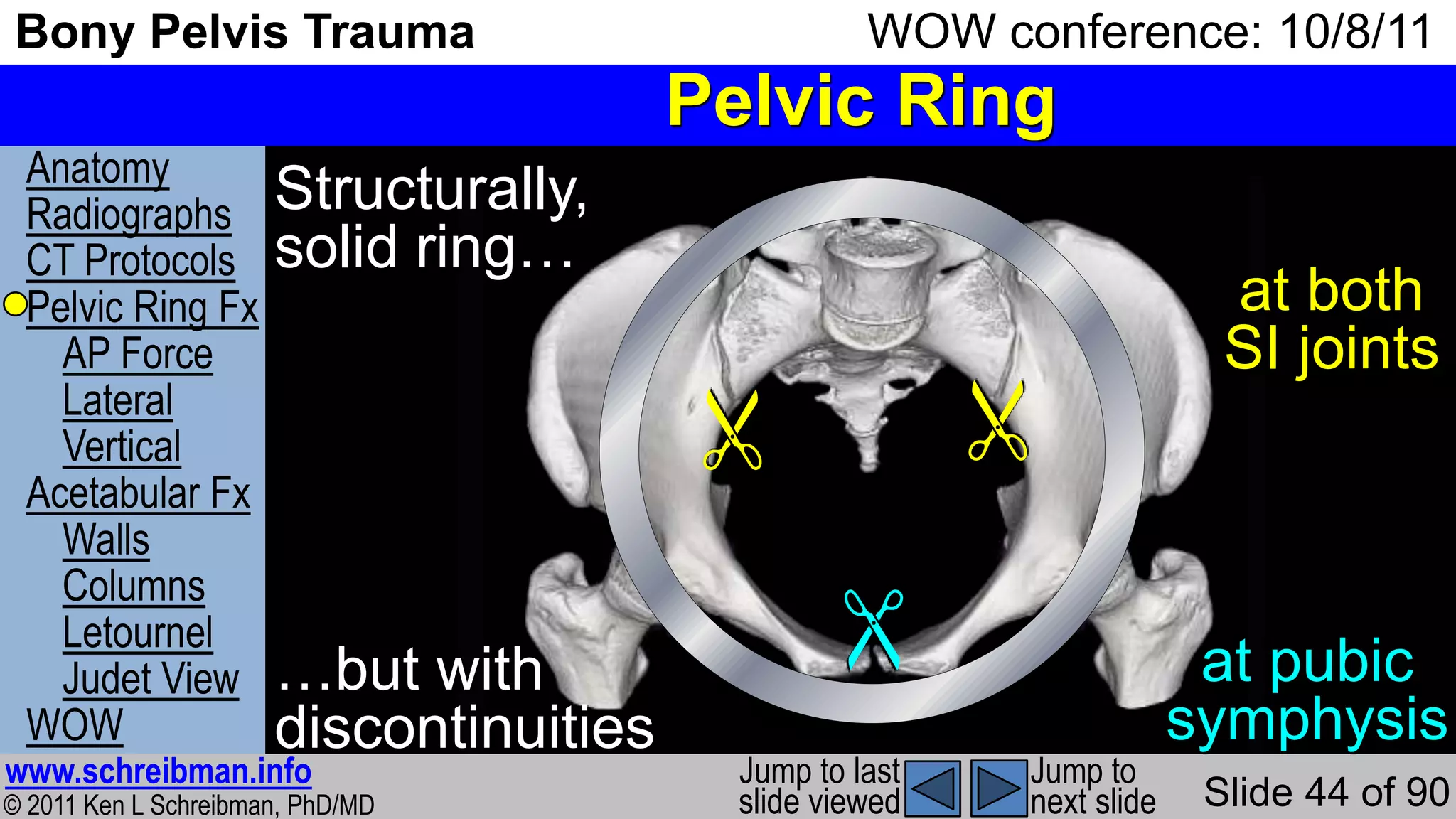















































The document presents an overview of the anatomy, radiographic protocols, and management strategies for pelvic injuries and femoral neck fractures. It highlights different views for imaging the pelvis and hip, emphasizing their importance in diagnosing conditions such as fractures and arthritis. Additionally, it discusses treatment methods, including percutaneous pinning and the implications of non-displaced versus displaced femoral neck fractures.























































































