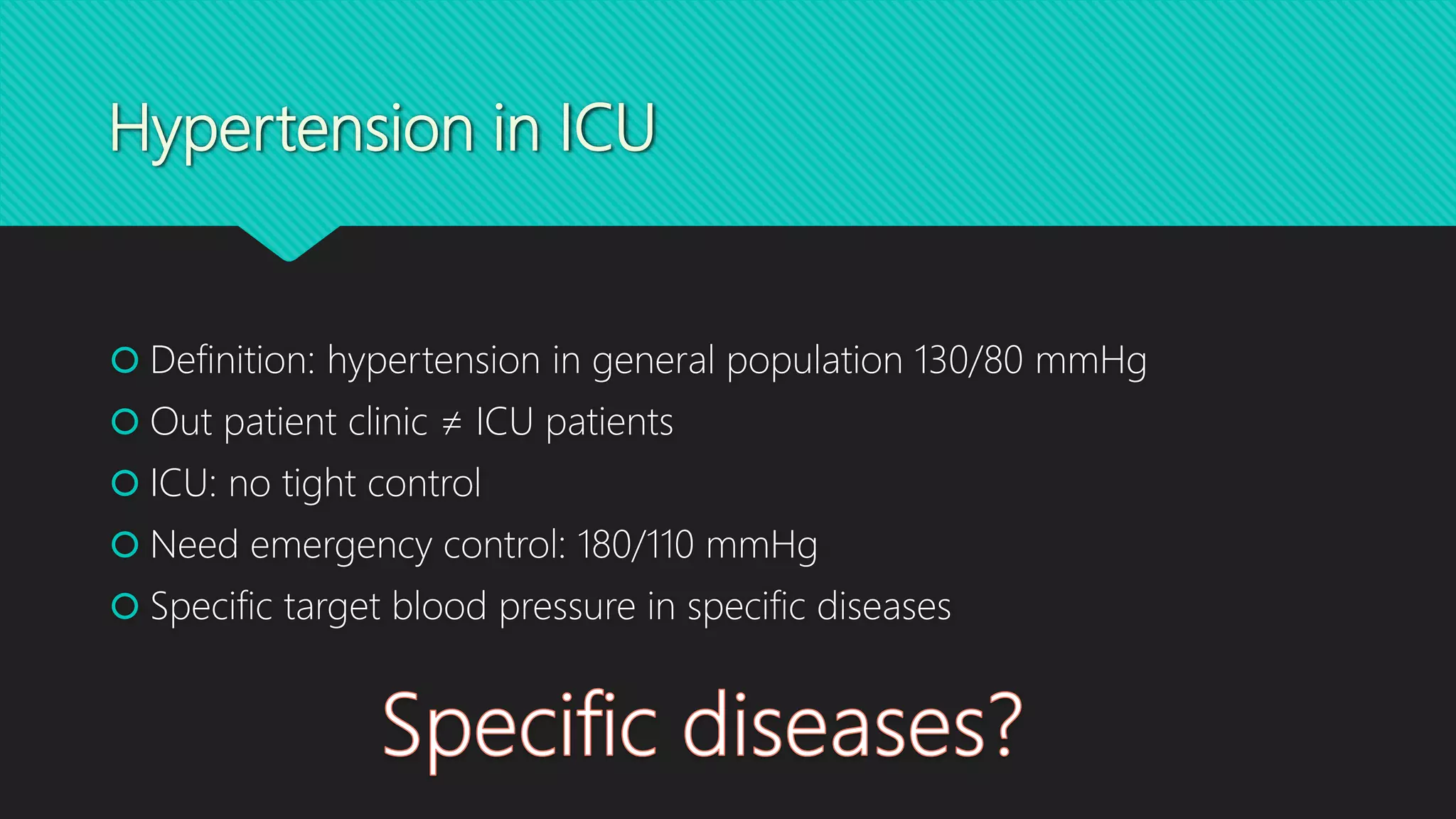
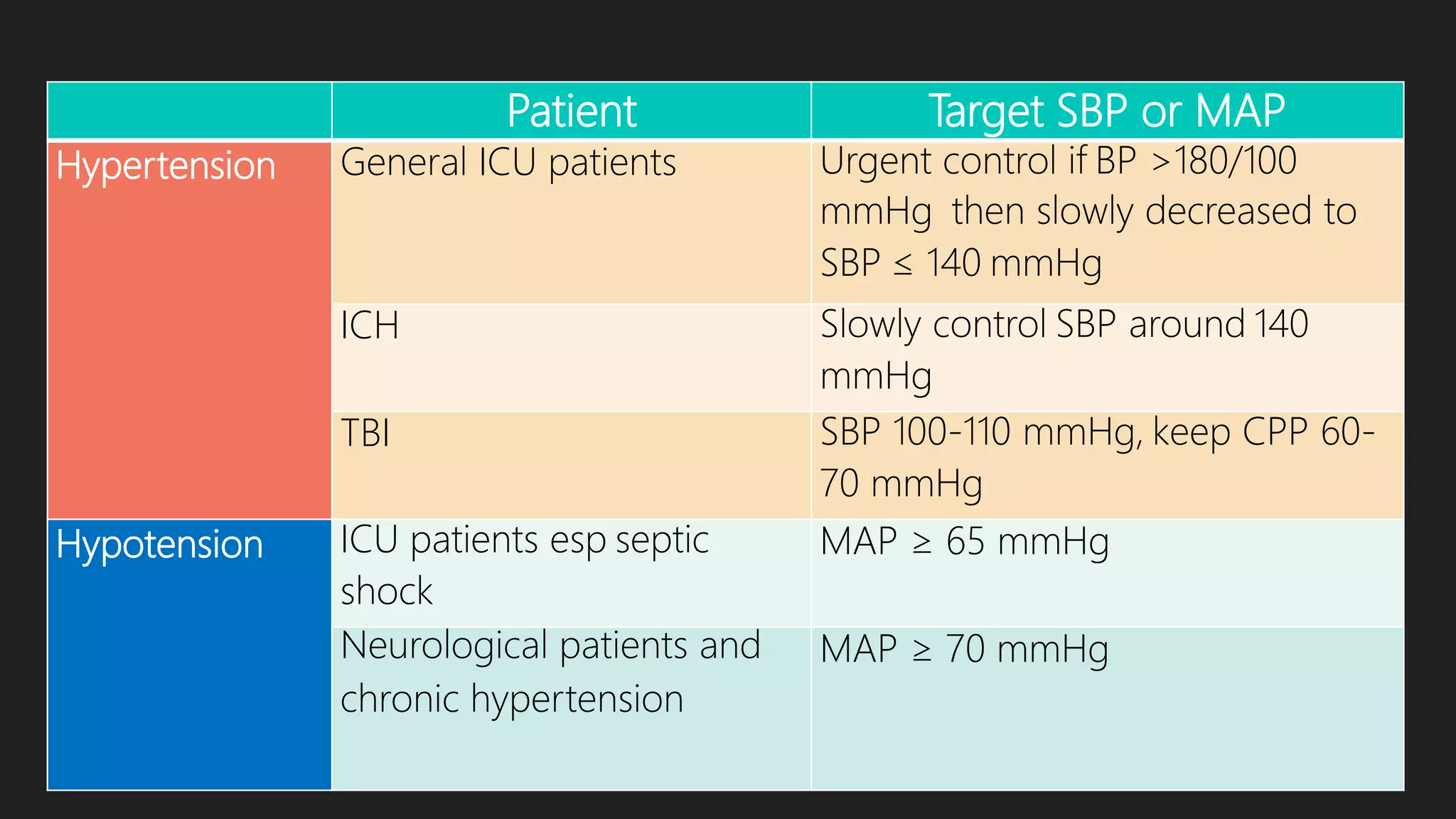
1) For general ICU patients, the target mean arterial pressure (MAP) is 75-100 mmHg, with hypertension defined as MAP over 180/110 mmHg and hypotension defined as MAP below 75 mmHg.
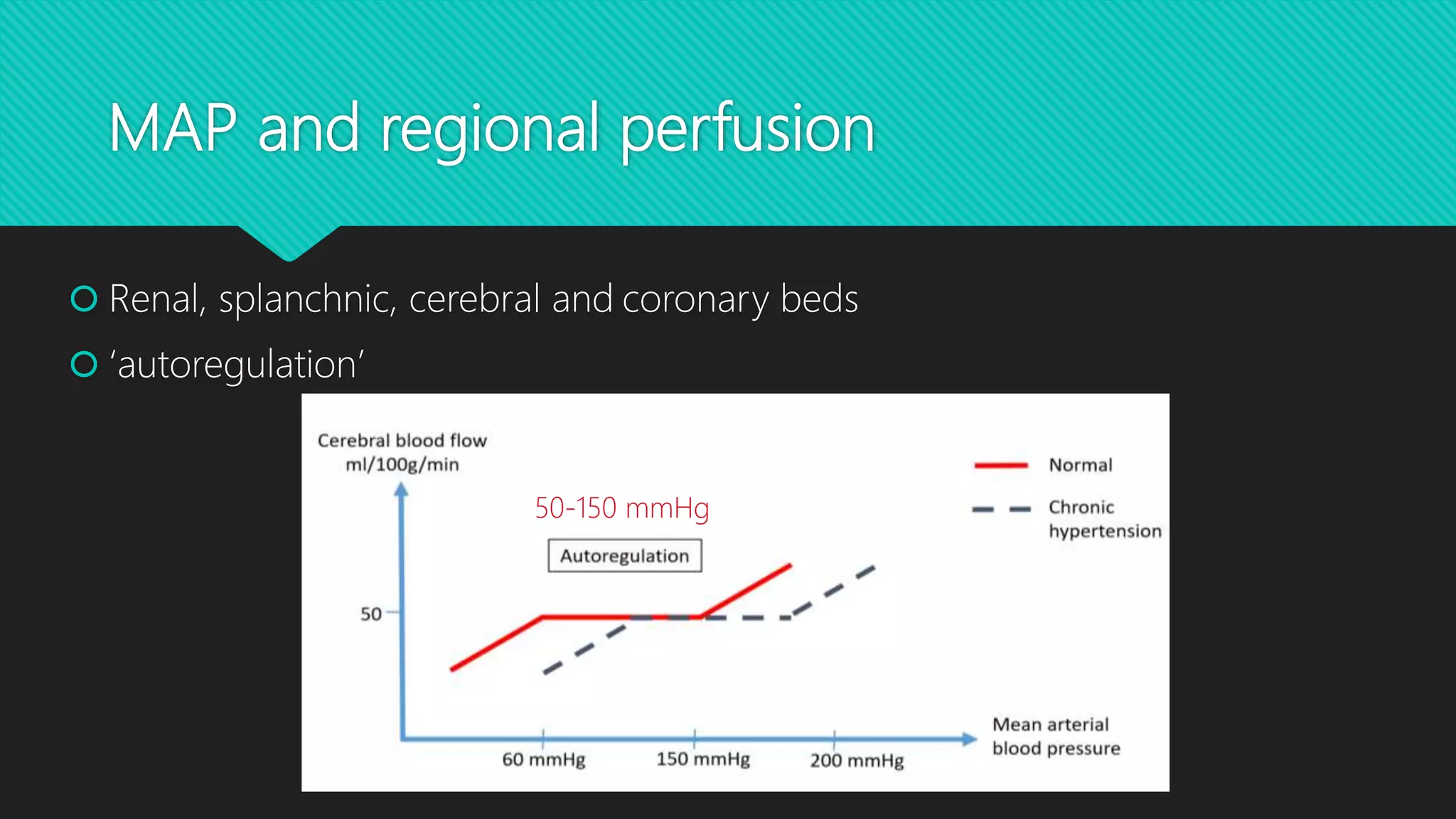
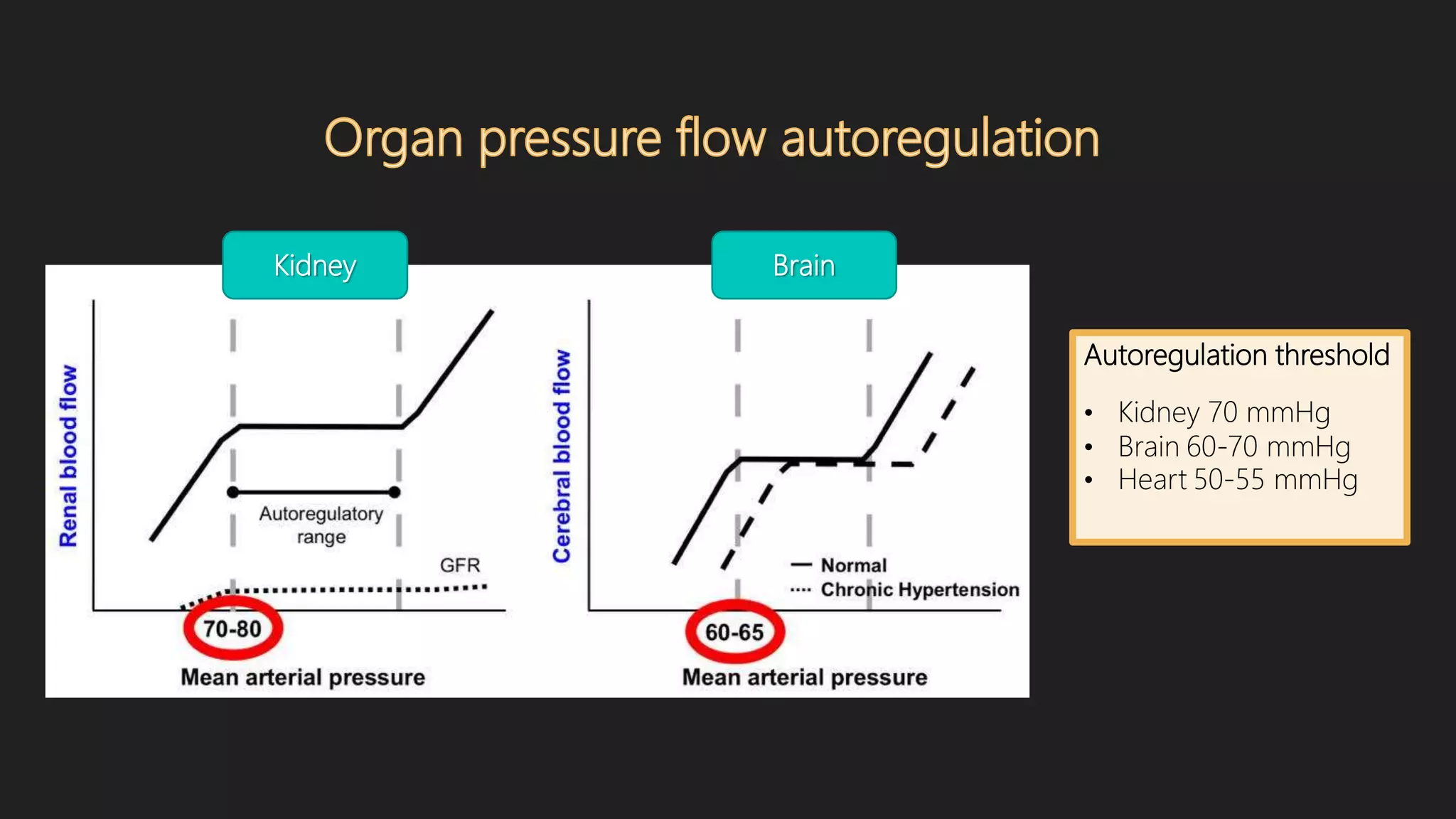
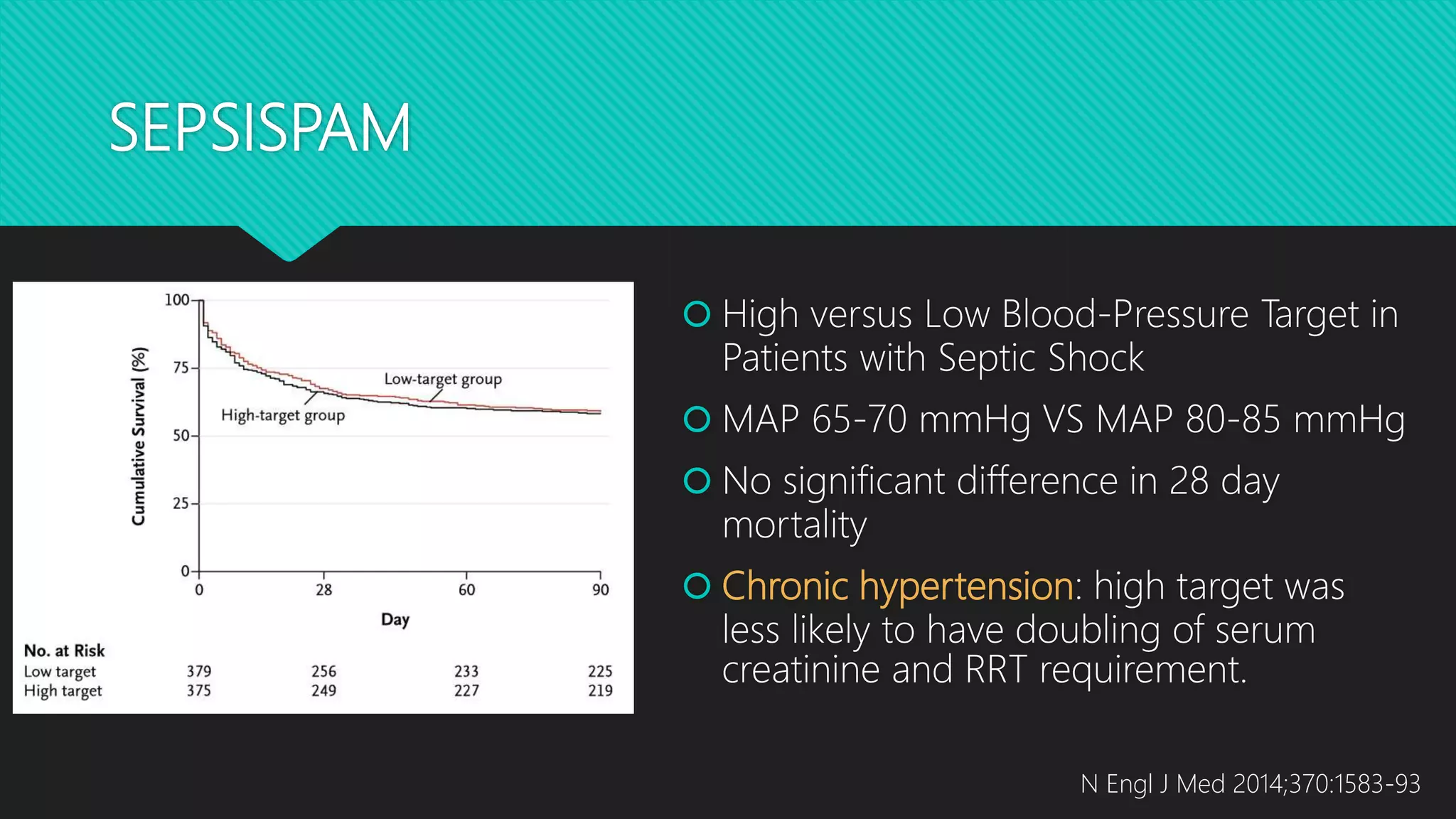
2) Blood pressure targets may need to be individualized based on a patient's specific condition and needs. For example, septic shock patients can often tolerate a lower MAP of 65-70 mmHg while neurological patients and those with chronic hypertension may need a higher MAP of at least 70 mmHg.
3) Precise blood pressure management is important as both overly high and low pressures can impact organ perfusion and outcomes. Factors like a patient's baseline blood pressure and individual response to medications
![MAP and Oxygen delivery
RA LA
RV LV
CVP
MAP
Cardiac
output
Venous
return
Pulmonary circulation
Systemic capillary
bed
DO2 = cardiac output x [(1.39 x Hb x SaO2) + (PaO2x 0.003)]](https://image.slidesharecdn.com/bloodpressuretargetinicu-180524032842/75/Blood-pressure-target-in-icu-5-2048.jpg)



















![Ambulatory blood pressure monitoring [abpm]](https://cdn.slidesharecdn.com/ss_thumbnails/ambulatorybloodpressuremonitoringabpm-140314094820-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)















![Esc guideline for atrial fibrillation 2020 [dr pranab]](https://cdn.slidesharecdn.com/ss_thumbnails/escguidelineforatrialfibrillationdrpranab-210919192333-thumbnail.jpg?width=640&height=640&fit=bounds)

















































