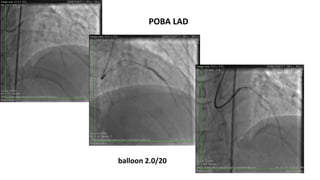
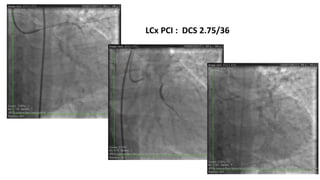
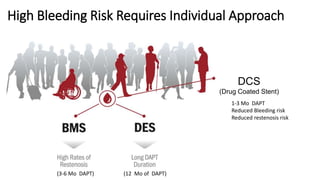
The document summarizes a case study of a high bleeding risk patient who required urgent PCI prior to orthopedic surgery. The patient had multiple vessel disease including chronic total occlusions. The interventional cardiologist performed complex PCI using dual guidewires and drug-coated stents, which allowed for a shortened dual antiplatelet therapy duration of 1 month prior to surgery. The case highlights the importance of an individualized approach for high bleeding risk PCI patients, including consideration of drug-coated stents to balance risks of bleeding and restenosis.