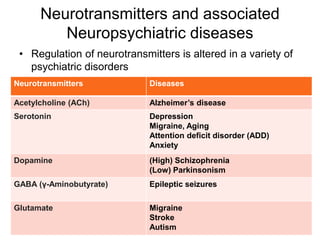
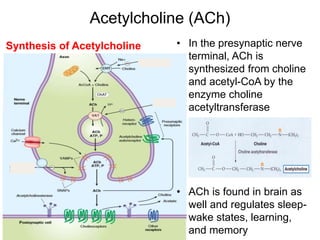
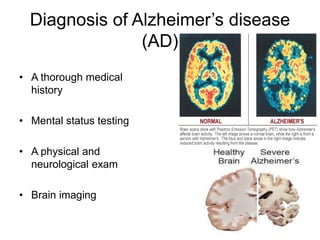
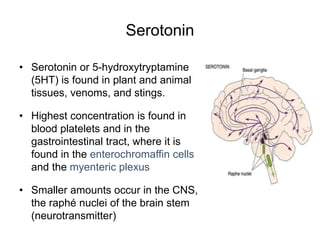
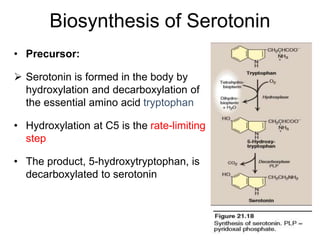
This document discusses the role of neurotransmitters in neuropsychiatric disorders. It begins by defining neuropsychiatry and describing common neuropsychiatric symptoms. It then focuses on two specific neurotransmitters - acetylcholine and serotonin. For acetylcholine, it describes its role in Alzheimer's disease, the stages of Alzheimer's, and treatments. For serotonin, it discusses its role in depression, migraine, biosynthesis, receptors, and treatments for depression.