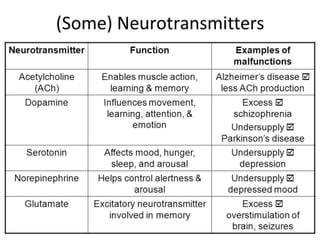
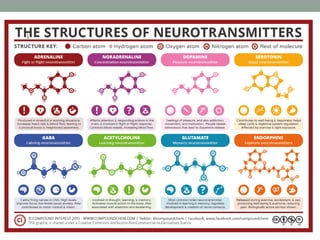
The document outlines objectives related to psychopharmacology, including the identification and discussion of various classes of psychotropic medications such as antidepressants, mood stabilizers, anxiolytics, and antipsychotics, along with their indications and side effects. It delves into neurobiological theories of mental disorders and the role of neurotransmitters like dopamine, serotonin, and norepinephrine in psychiatric conditions and medication effects. Additionally, it includes guidelines for pharmacological strategies, monitoring, and treatment options for different mood disorders.







![159
Benzodiazepines
• Ideal for management of withdrawal symptoms
• Cross-tolerance with alcohol
• Fairly wide therapeutic window
• Short- vs. long-acting
• diazepam [5-20 mg p.o. every 4-6 hour, starting dose of
10-30 mg i.v. if needed],
• chlordiazepoxide –
• avoid in intoxication and long-term use, risk of respiratory
depression and sedation
• Liver disease limits use to short acting medications
without active metabolites](https://image.slidesharecdn.com/psychopharmacology-231019022733-fd210d59/85/Psychopharmacology-pptx-159-320.jpg)
![Treatment of withdrawal
• Beta blockers (e.g. propranolol or atenolol for
autonomic hyperactivity)
• Valproate or carbamazepine - if seizures are
present
• Haloperidol - for hallucinations, delusions,
and violence in delirium [5-10 mg p.o. or i.m.],
together with benzodiazepines (risk of
seizures and extrapyramidal side effects)](https://image.slidesharecdn.com/psychopharmacology-231019022733-fd210d59/85/Psychopharmacology-pptx-165-320.jpg)