Download as PDF, PPTX
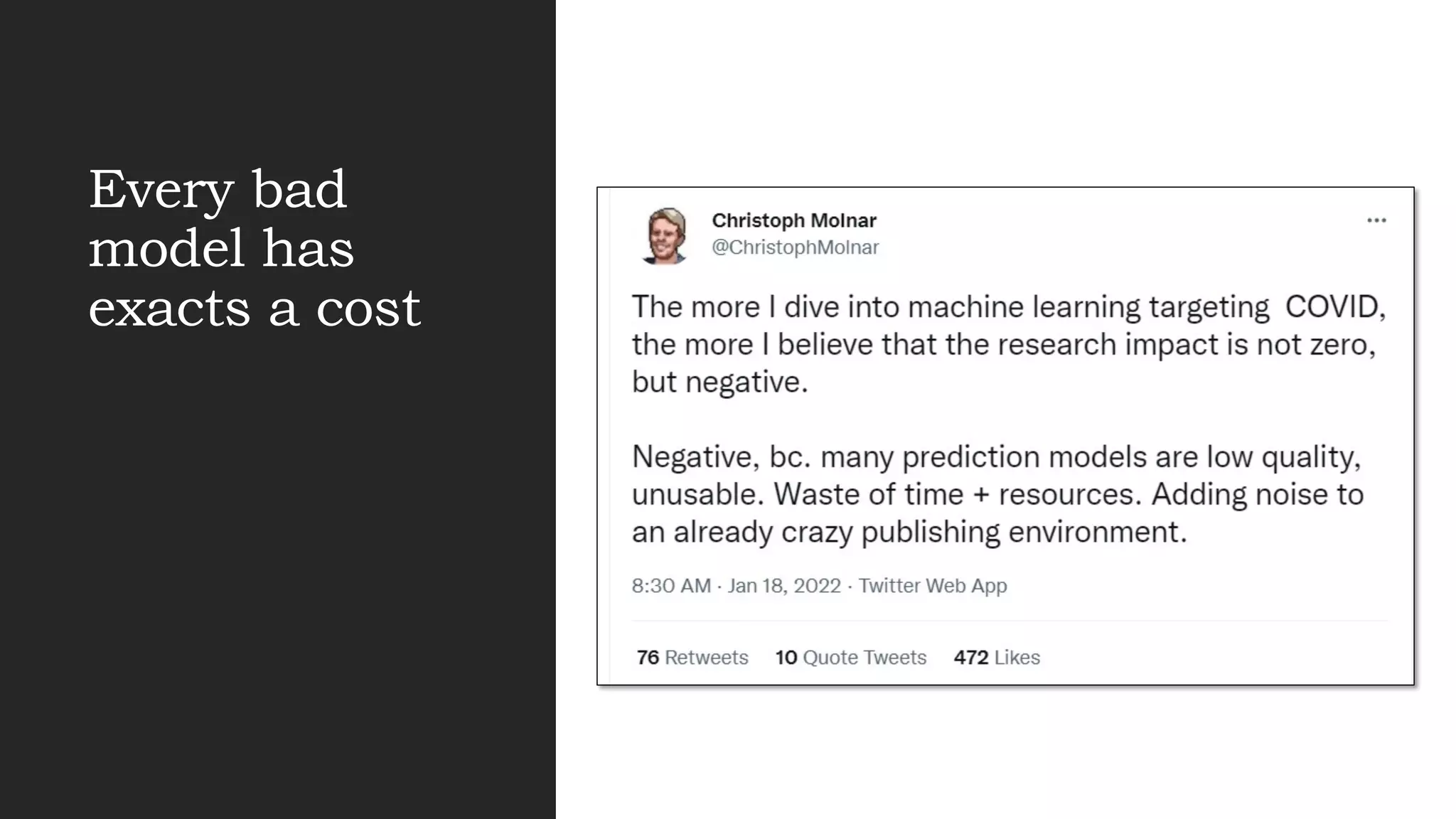
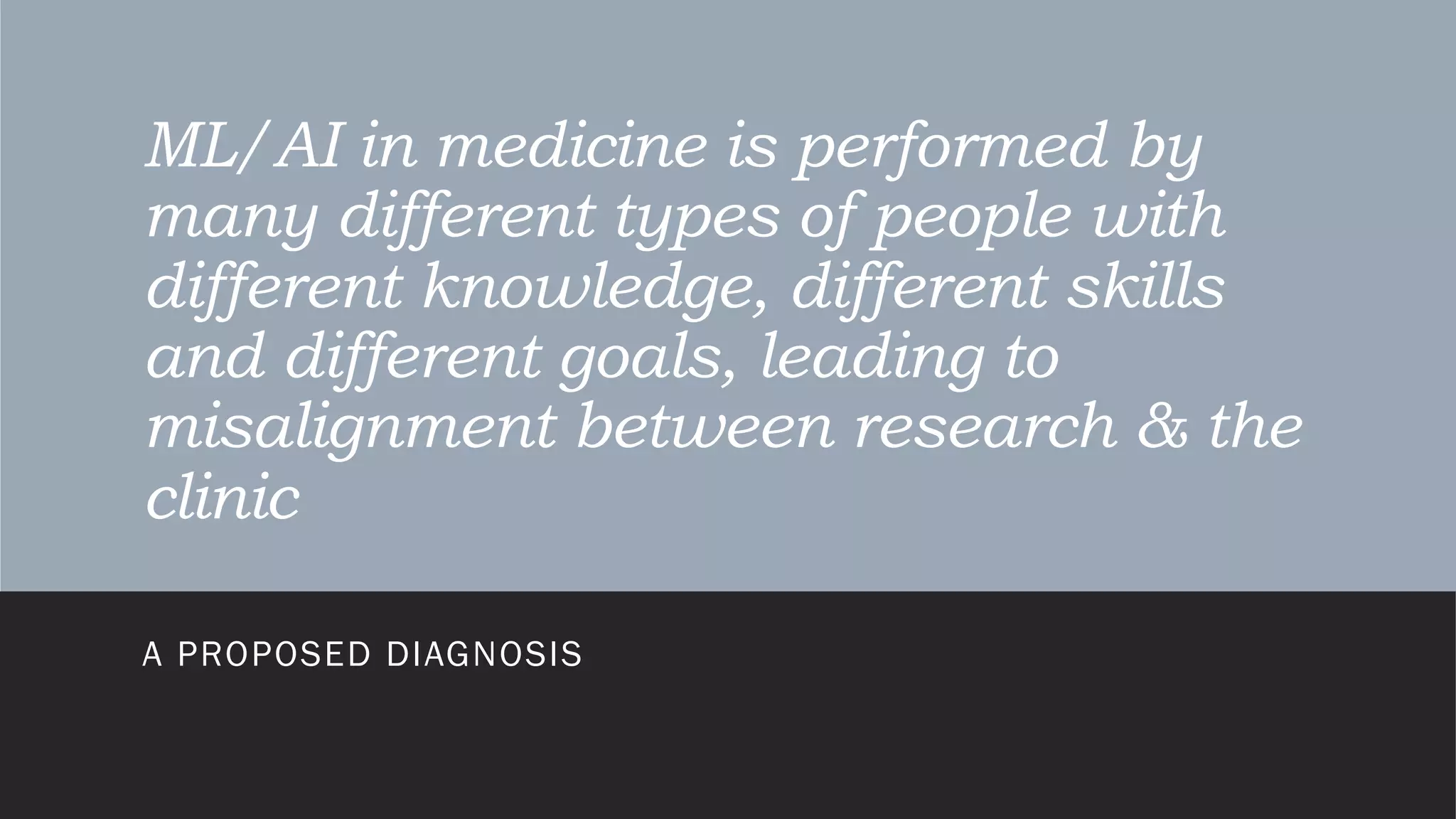
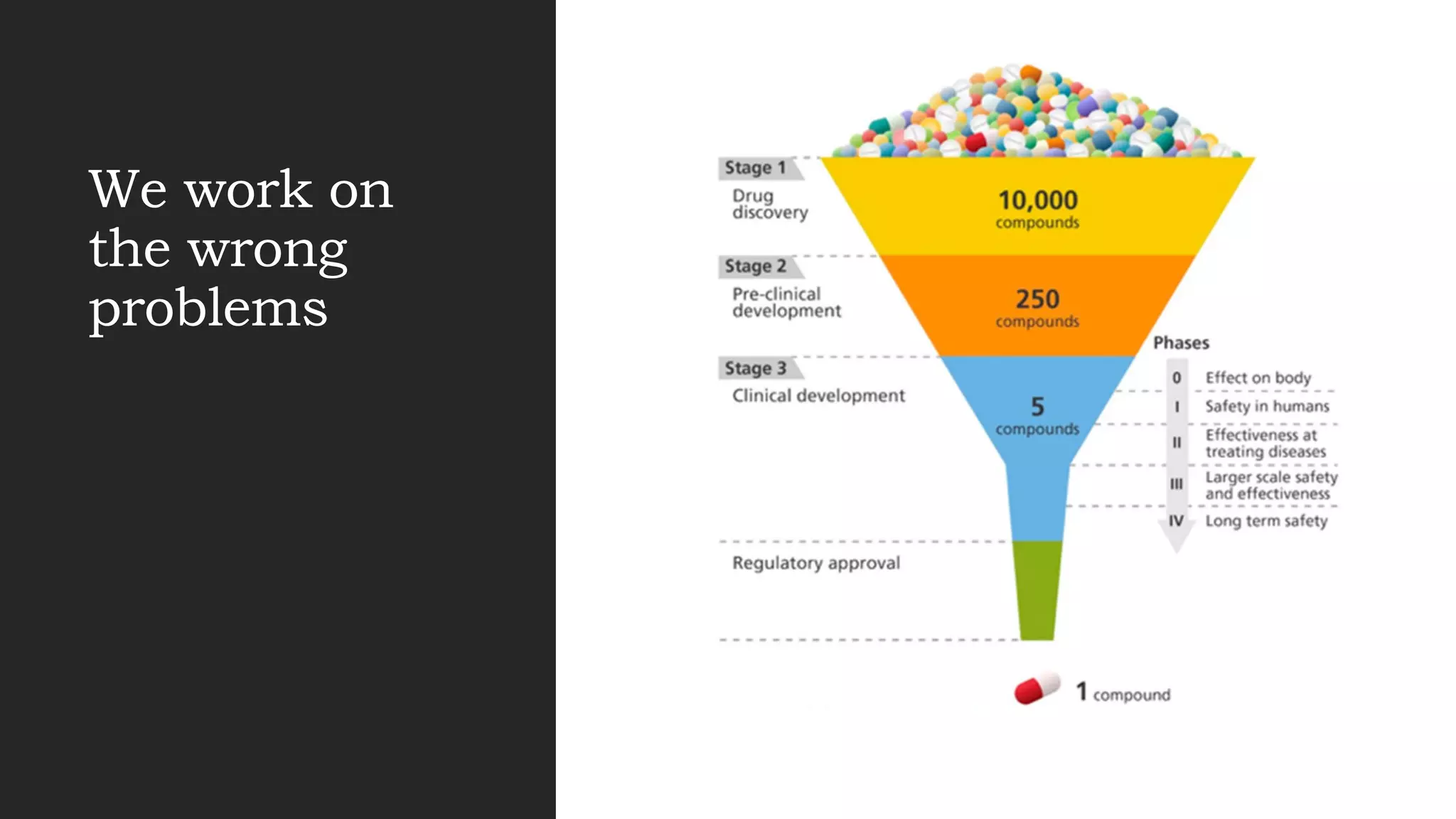
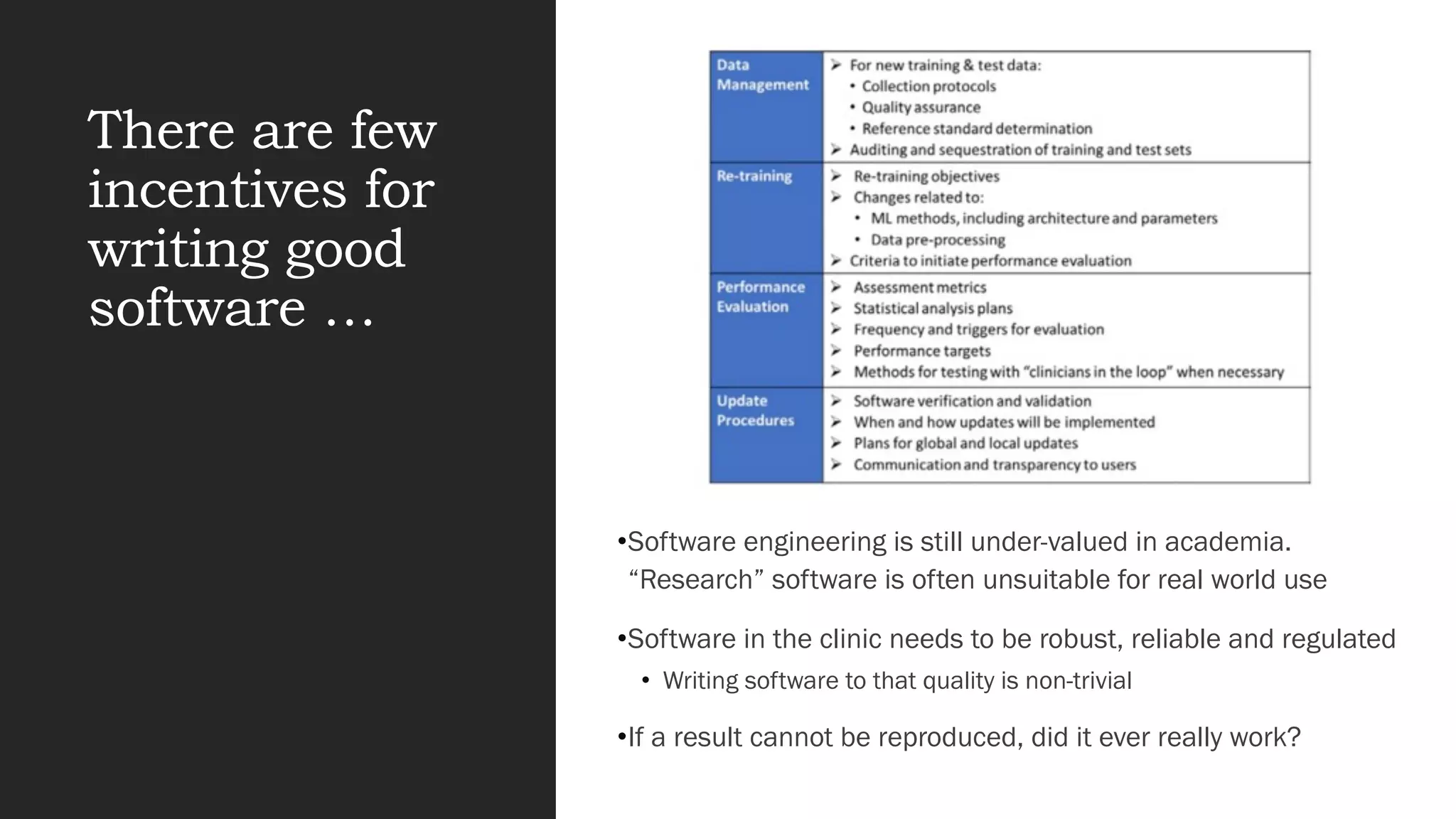


This document discusses challenges with applying machine learning and AI to healthcare and biomedicine. It summarizes that while AI promises improvements, many projects fail to deliver due to issues like focusing on the wrong problems, lack of data, and lack of collaboration between fields. It advocates for approaches like validating and reproducing results, ensuring interpretability, collaborating across expertise, and focusing on incremental improvements rather than novel methods alone.


































![[DSC Europe 23][DigiHealth] Dimitrios Kalogeropoulos A Sustainable Future for...](https://cdn.slidesharecdn.com/ss_thumbnails/3xzq6p1qtg65y98lodrk-dimitrios-231130112725-689fcaa2-thumbnail.jpg?width=640&height=640&fit=bounds)



















































