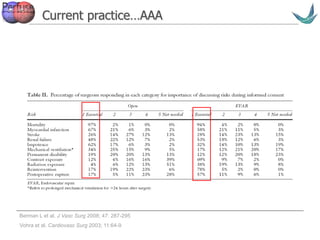
1) The document discusses the evolving standards for informed consent in medical procedures, moving from a professional standards approach to a reasonable patient standard that requires disclosure of all material risks.
2) Ensuring patient understanding of medical procedures and risks is challenging, as multiple factors like timing, education level, and context can influence comprehension.
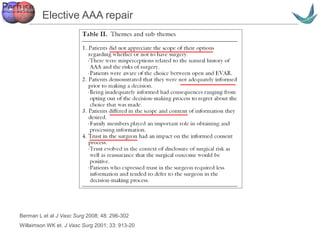
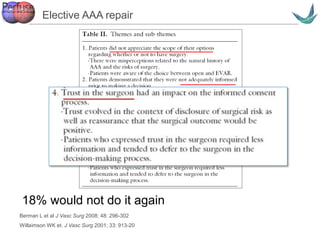
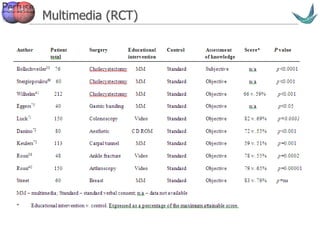
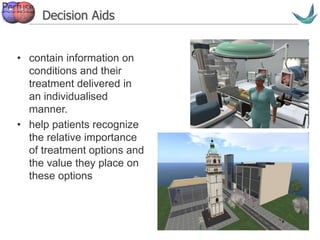
3) Effective consent requires an ongoing process of discussion tailored to individual patient needs that incorporates written information, multimedia tools, and shared decision making to build trust and understanding.


![Vascular surgery @ Tallaght
Professional standards approach
• Bolam standards (1957)
• Sidaway: “An issue whether nondisclosure of
a particular risk or cluster of risks in a
particular case should be condemned as a
breach of the doctor’s duty of care is an issue
to be decided on the basis of expert medical
evidence.”1
11. Sidaway v Board of Governors of the Bethlem Royal Hospital [1985]](https://image.slidesharecdn.com/beyondconsent-161107164731/85/Beyond-consent-10-320.jpg)

![Vascular surgery @ Tallaght
Ireland - 1992
• Orchialgia after vasectomy
• The Chief Justice favoured the
application of the ‘professional standard
approach’, while other members
favoured the ‘reasonable patient test’
James Walsh Family Planning Services Ltd & ors [1992] IR 496](https://image.slidesharecdn.com/beyondconsent-161107164731/85/Beyond-consent-12-320.jpg)
![Vascular surgery @ Tallaght
Ireland - 2000
• Neuralgia after dental surgery
• Expert witnesses would not have
warned the patient
Peter Geoghegan v David Harris [2000] IR 536 Justice Kearns
• In such an elective procedure, the practitioner
must disclose all known risks, of grave
consequence or severe pain, no matter how
remote. This would ensure that the patient could
make a "real" choice.](https://image.slidesharecdn.com/beyondconsent-161107164731/85/Beyond-consent-13-320.jpg)
![Vascular surgery @ Tallaght
Ireland - precedent
• Elective operation
– Patient did not need the operation and the proposed
benefits did not, in his view, outweigh the detriment
which occurred.
• The complication was not minor or trivial
(however rare)
– obligation to disclose complications resulting in
grave consequence or severe pain is reasonable.
• Patient is the arbiter of whether a risk is
acceptable
Peter Geoghegan v David Harris [2000] IR 536 Justice Kearns](https://image.slidesharecdn.com/beyondconsent-161107164731/85/Beyond-consent-14-320.jpg)
![Vascular surgery @ Tallaght
Ireland - 2007
• Diplopia after squint surgery
• Whether patient was fully informed
• Consent on the morning of surgery
Fitzpatrick -v- White, [2007] IESC 51 (2007) Justice Kearns
• “in the context of elective surgery, a warning given only
shortly before an operation is undesirable. The patient
may be stressed, medicated or in pain, and may be less
likely for one or more of these reasons to make a calm
and reasoned decision.”](https://image.slidesharecdn.com/beyondconsent-161107164731/85/Beyond-consent-15-320.jpg)

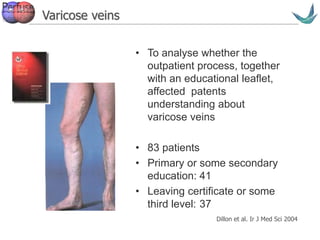


![Vascular surgery @ Tallaght
“… there is no evidence that information leaflets
enhance understanding in this [clinical trials]
patient group…”
Information leaflets
Ryan et al 2008](https://image.slidesharecdn.com/beyondconsent-161107164731/85/Beyond-consent-41-320.jpg)




















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















