
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Basic ecg
Similar to Basic ecg (20)
Recently uploaded
Recently uploaded (20)
Basic ecg
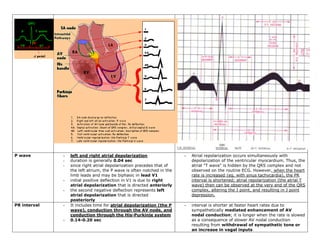
- 1. P wave - left and right atrial depolarization - Atrial repolarization occurs simultaneously with - duration is generally 0.04 sec depolarization of the ventricular myocardium. Thus, the - since right atrial depolarization precedes that of atrial "T wave" is hidden by the QRS complex and not the left atrium, the P wave is often notched in the observed on the routine ECG. However, when the heart limb leads and may be biphasic in lead V1 rate is increased (eg, with sinus tachycardia), the PR - initial positive deflection in V1 is due to right interval is shortened; atrial repolarization (the atrial T atrial depolarization that is directed anteriorly wave) then can be observed at the very end of the QRS - the second negative deflection represents left complex, altering the J point, and resulting in J point atrial depolarization that is directed depression. posteriorly PR interval - It includes time for atrial depolarization (the P - interval is shorter at faster heart rates due to wave), conduction through the AV node, and sympathetically mediated enhancement of AV conduction through the His-Purkinje system nodal conduction; it is longer when the rate is slowed - 0.14-0.20 sec as a consequence of slower AV nodal conduction resulting from withdrawal of sympathetic tone or an increase in vagal inputs
- 2. QRS complex - ventricular depolarization - the negative deflection following the R wave is the S - 0.06 to 0.10 seconds (2 1/2 small boxes) wave which represents terminal depolarization of the and is not influenced by heart rate high lateral wall - An initial negative deflection is the Q wave due - If there is a second positive deflection it is known as to septal depolarization an R'. - The first positive deflection isthe R wave which - Lower case letters (q, r, or s) are used for relatively represents depolarization of the left ventricular small amplitude waves of less then 0.5 mV (less than 5 myocardium mm with standard calibration) - Right ventricular depolarization is obscured - An entirely negative QRS complex is called a QS wave. because the left ventricular myocardial mass is much greater than that of the right ventricle. ST segment - The ST segment occurs after ventricular - In disease states, ST segment may be horizontally depolarization has ended and before depressed (below the isoelectric line), elevated in a repolarization has begun concave or convex direction (above the isoelectric line), - It is a time of electrocardiographic silence or downsloping. - The initial part of the ST segment is termed the J point. T wave - ventricular repolarization - depolarization begins at the endocardial surface and - Since the rate of repolarization is slower than spreads to the epicardium while repolarization begins depolarization, the T wave is broad, has a slow at the epicardial surface and spreads to the upstroke, and rapidly returns to the isoelectric endocardium, the direction or vector of ventricular line following its peak depolarization is opposite to that of ventricular repolarization. Thus, the T wave direction or vector on the ECG normally is in the same direction as the QRS QT interval - primarily a measure of membrane repolarization - a QT interval that is corrected for heart rate (QTc) is - The time for ventricular repolarization and often calculated as follows: therefore the QT (or JT) interval is dependent upon the heart rate; it is shorter at faster heart QTc = QT interval ÷ square root of the RR interval (in sec) rates and longer when the rate is slower - 0.44 sec U wave - seen in right precordial leads V2 to V4 - The U wave may merge with the T wave when the QT - represents delayed repolarization of the His- interval is prolonged (a QT-U wave), or may become Purkinje system very obvious when the ST interval (and hence QT or JT - Alternatively, it may represent a mechanical interval) is shortened (eg, with digoxinor event such as ventricular relaxation hypercalcemia) - typically less than 0.2 mV - more evident in some circumstances s/a hypokalemia