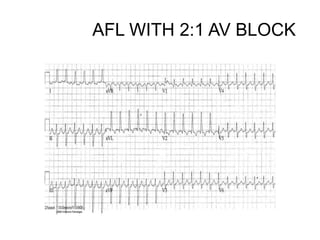
2. ATRIAL FLUTTER WITH 2:1
BLOCK
• There is a narrow complex tachycardia at 150 bpm.
• There are no visible P waves.
• There is a sawtooth baseline in V1 with flutter waves visible at
300 bpm.
• Elsewhere, flutter waves are concealed in the T waves and QRS
complexes.
• The heart rate of 150 bpm makes this flutter with a 2:1 block.
• NB. Flutter waves are often very difficult to see when 2:1 block is
present.
• Remember
• Suspect atrial flutter with 2:1 block whenever there is a regular
narrow-complex tachycardia at 150 bpm — particularly when
the rate is extremely consistent.
• In contrast, the rate in sinus tachycardia typically varies slightly
from beat to beat, while in AVNRT/AVRT the rate is usually faster
(170-250 bpm).
• To tell the difference between these rhythms, try some vagal
manoeuvres or give a test dose of adenosine — AVNRT/AVRT will
5. 3:1 AV BLOCK [CONSTANT PR
INTERVAL WITH VENTRICULAR
CONDUCTED BEAT]
6. SINUS ARREST WITH: V-
ESC-RHYTHM
BLUE ARROWS: ‘P’ WAVES
DUE TO RETROGRADE
CONDUCTION.
7. • In ventricular escape beat or rhythm, the
depolarization wave spreads slowly via
abnormal pathway in the ventricular
myocardium and not via the His bundle and
bundle branches. Therefore, the QRS
complex is wide (>120 ms) and has a shape
different from that of the sinus beat. If the
ventricular escape rhythm is the result of
sinus node failure, no P wave of atrial
contraction is seen as in the tracing above. If
the ventricular escape rhythm is the result
of 3rd degree (complete) heart block, the
sinus node paces the atria independently
10. • In junctional (AV junctional) beat or rhythm
the atrial depolarization current points
cephalad and to the right, away from lead II
and toward lead aVR. Therefore the P wave,
if seen, would be negative in lead II and
positive in lead aVR. However this P wave is
usually buried by the QRS complex and not
visible. On less common occasions when the
P wave is visible, it may be either
immediately before or immediately after the
QRS complex. Since the impulse is
conducted to the ventricles via the His
bundle and bundle branches, the QRS
13. RETROGRADE ‘P’ WAVES
NOTE:
If there is Coexistent AV Block
along with Sinus Arrest
Retrograde ‘P’ waves will not be
present along with the Escape
Rhythm.
14. Hindawi Publishing Corporation Case
Reports in Cardiology Volume 2016,
Article ID 7919642, 3 pages
http://dx.doi.org/10.1155/2016/791
9642
Case Report :Torsade de Pointes Triggered by
Early Ventricular Escape Beats in a Patient
with Complete Atrioventricular Block Erkan
Yildirim,1 Baris Bugan,2 Suat Gormel,1 Uygar
Cagdas Yuksel,1 Murat Celik,1 Yalcin
Gokoglan,1 Serdar Firtina,1 Sinan Iscen,1 Emre
Yalcinkaya,1 Ugur Kucuk,1 and Hasan Kutsi
Kabul1 1 Department of Cardiology, Gulhane
Military Medical Academy, 06010 Ankara,
15. 1. Syncope is a frequent symptom in
patients with complete atrioventricular
block (CAVB) [1]. In the majority of cases,
low cardiac output caused by decreased
heart rate is responsible for the
symptoms. However in some cases
bradycardia associated QT prolongation
may lead to malignant ventricular
tachyarrhythmias causing syncope [1,
2]. We, herein, reported a case with
CAVB complicated with frequent
16. • In conclusion, acquired CAVB may
sometimes induce TdP and the
episodes of TdP result in syncope,
cardiac arrest, and even death due
to degeneration into ventricular
fibrillation. PVCs especially “R-on-
T” phenomenon should alert
physicians as precursors for
ventricular fibrillation and sudden
death. Early recognition and